
Shoulder Exam (Benchmark)
Benchmarks for a problem focused exam of a patient with shoulder pain include:
Inspection
- Anterior, lateral and posterior shoulder
Palpation
- Palpate systematically, noting warmth, deformity, swelling and tenderness:
- Sternoclavicular joint
- Clavicle
- Acromioclavicular (AC) joint
- Biceps tendon in the bicipital groove
- Subacromial space and rotator cuff:
- Supraspinatus tendon
- Infraspinatus tendon
- Teres minor
- Subscapularis insertion
- Scapula
- Coracoid process
Range of motion
- Flexion, also called forward elevation
- Abduction
- Internal and external rotation
Strength Testing
- Flexion/forward elevation and extension
- Abduction and adduction
- Internal and external rotation
Stability and Special Tests (as directed by DDx)
- If you suspect rotator cuff dysfunction:
- Perform targeted strength testing of rotator cuff muscles:
- Empty can test
- Lift off test
- Assess for bursitis or impingement
- Neer test
- Hawkins test
- Perform targeted strength testing of rotator cuff muscles:
- If you suspect biceps pathology: Speed’s test
- If you suspect joint instability or laxity: Apprehension sign and relocation sign
Key landmarks & structures
Identify each of the following landmarks, moving from anterior to lateral to posterior shoulder.
Spine landmarks can also be useful in your documentation of tenderness or ROM.
- C7 is the prominent “bump” in the lower neck
- T4 is at the spine of the scapula
- T7 is at the inferior pole of the scapula
- L4 vertebra is at the level of the iliac crests
Inspection
Inspect the anterior, lateral and posterior shoulder, observing for symmetry, swelling, erythema, ecchymosis, atrophy and muscle bulk.
Palpation
Palpate the shoulder systematically, starting with the sternoclavicular joint and moving systematically, from anterior to lateral to posterior.
-
- Sternoclavicular joint
- Clavicle
- Acromioclavicular (AC) joint
- Biceps tendon in the bicipital groove
- Coracoid process is the origin of the short head of the biceps
- Subacromial space and rotator cuff:
- supraspinatus tendon lies just below the anterior lateral acromion
- infraspinatus tendon lies just below posterolateral acromion
- teres minor lies just inferior to the infraspinatus
- subscapularis insertion lies just lateral to coracoid at the anterior shoulder
- Scapula:
- spine of the scapula is the origin of the infraspinatus
Range of motion
Assess active and passive ROM in each plane. If range of motion is limited, note whether it is limited by pain or “true” restriction. Adhesive capsulitis and glenohumeral arthritis limit or cause pain with both active and passive ROM. Injury of muscles or ligaments affect active more than passive ROM. Increased ROM of the shoulder suggests ligamentous laxity or prior dislocations.
You can also assess the shoulder with simple functional tests.
- Internal rotation and adduction: Ask your patient to reach up behind the back to touch the highest point on the spine that they can. This tests internal rotation and adduction. Normal shoulder ROM is to reach up to T10.
- External rotation and abduction: Ask your patient to reach as far down behind their head as they can to touch the spine. This tests external rotation and abduction. Normal shoulder ROM is to reach down to T1.
Strength testing
With your patient seated, test strength of shoulder flexion, extension, abduction, adduction, internal and external rotation, grading each movement on the 0-5 scale. If you suspect long thoracic nerve injury, you can test subscapularis strength by asking your patient to perform a ‘mini-push up’ against the wall and observing for scapular winging.
Hypothesis Driven Physical Exam
If you are concerned about a rotator cuff disorder
Rotator cuff disorders are common, and include tendinitis, tear, subacromial bursitis, and impingement syndromes. If you suspect rotator cuff pathology, there are many special tests you can perform, and different examiners prefer different maneuvers. The ones we would like you to practice in FCM are below.
Perform targeted strength testing of rotator cuff muscles
The rotator cuff is made up of the 4 ‘SITS’ muscles. Targeted testing of these muscles may reveal pain, which suggests tendinitis, or weakness, which supports a rotator cuff tear.
- Supraspinatus: abduction from 0 to 90 degrees
- Infraspinatus: external rotation
- Teres Minor: external rotation
- Subscapularis: internal rotation
![]() The Empty Can Test isolates the supraspinatus. The shoulder is held in 80 degrees of flexion, 45 degrees of abduction and full internal rotation, as if dumping out a can of soda. The provider places downward pressure on forearm as patient resists. Weakness or pain support supraspinatus tendinitis or tear.
The Empty Can Test isolates the supraspinatus. The shoulder is held in 80 degrees of flexion, 45 degrees of abduction and full internal rotation, as if dumping out a can of soda. The provider places downward pressure on forearm as patient resists. Weakness or pain support supraspinatus tendinitis or tear.
 The Lift Off Test isolates the subscapularis. With the shoulder fully internally rotated behind the back, the patient attempts to push their arm off back against resistance from the examiner. Weakness or pain support subscapularis tendinitis or tear.
The Lift Off Test isolates the subscapularis. With the shoulder fully internally rotated behind the back, the patient attempts to push their arm off back against resistance from the examiner. Weakness or pain support subscapularis tendinitis or tear.
Special tests for rotator cuff impingement or bursitis
 Neer test: The shoulder is guided through full flexion and abduction with stability held on the scapula. Pain is considered a positive finding.
Neer test: The shoulder is guided through full flexion and abduction with stability held on the scapula. Pain is considered a positive finding.
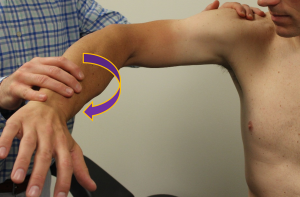 Hawkins/Kennedy test: The shoulder is held in 90 degrees of flexion with the elbow flexed, as if a hawk were perched on the forearm. The shoulder is then forcibly internally rotated, with pain considered a positive finding.
Hawkins/Kennedy test: The shoulder is held in 90 degrees of flexion with the elbow flexed, as if a hawk were perched on the forearm. The shoulder is then forcibly internally rotated, with pain considered a positive finding.
Other findings of rotator cuff disease
 Visible atrophy suggests longstanding rotator cuff disease. Decreased muscle mass in the suprascapular fossa suggests atrophy of the supraspinatus, the most commonly involved rotator cuff muscle in rotator cuff disorders. Infraspinatus atrophy can also be seen in this image.
Visible atrophy suggests longstanding rotator cuff disease. Decreased muscle mass in the suprascapular fossa suggests atrophy of the supraspinatus, the most commonly involved rotator cuff muscle in rotator cuff disorders. Infraspinatus atrophy can also be seen in this image.
If you are concerned about a biceps tendon injury: Speed’s test
Biceps tendon injuries can range from from mild tendinopathy to complete tendon rupture.
 To assess for biceps pathology, perform Speed’s test. The shoulder is held at 90 degrees of flexion with the forearm in supination and the patient resists pressure from the examiner. Weakness or pain supports biceps pathology.
To assess for biceps pathology, perform Speed’s test. The shoulder is held at 90 degrees of flexion with the forearm in supination and the patient resists pressure from the examiner. Weakness or pain supports biceps pathology.
If you are concerned about shoulder instability
Stability of the shoulder is a complex system, and testing primarily evaluates for previous subluxation and dislocation. Most dislocations occur anteriorly and happen when the shoulder is in abduction and external rotation. Hold up your arm as if you’re throwing a ball – this position puts the shoulder in the position of maximal stress.
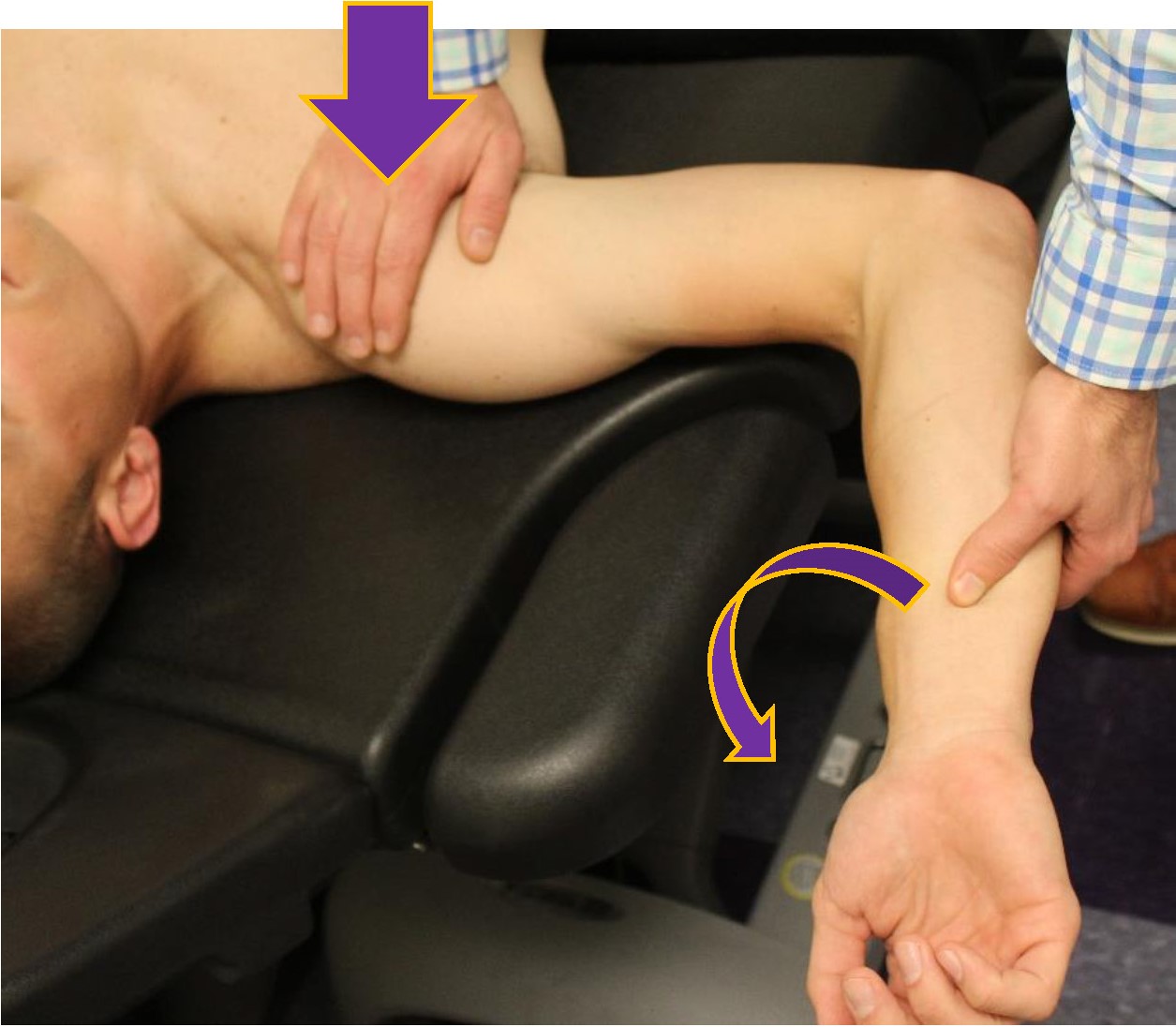
 The apprehension test assesses for subluxation by placing the shoulder in the position of maximum risk and applying further stress. Passively place the patient’s arm in 90 degrees of abduction, 90 degrees of elbow flexion, and 90 degrees of external rotation. The examiner then attempts to push the shoulder into further external rotation.
The apprehension test assesses for subluxation by placing the shoulder in the position of maximum risk and applying further stress. Passively place the patient’s arm in 90 degrees of abduction, 90 degrees of elbow flexion, and 90 degrees of external rotation. The examiner then attempts to push the shoulder into further external rotation.
A positive apprehension sign is that the patient is apprehensive or will not allow the examiner to put the arm in this position. This indicates that the patient has anterior instability that could allow shoulder dislocation.
The relocation test is performed if the apprehension test is positive, repeating the stress of the apprehension test while holding pressure on the anterior glenohumeral joint. This pressure prevents the ball of the humerus from dislocating anteriorly, and typically reduces pain and apprehension in those with subluxation or past dislocation.