
Hip Exam
Inspect:
- Anterior, lateral and posterior hip
- Observe for antalgia and functional range of motion while walking.
Palpate: systematically from anterior to lateral to posterior, noting warmth, deformity, swelling, tenderness
Range of motion:
- Flexion and extension
- Adduction and abduction
- Internal rotation and external rotation
Strength:
- With the patient supine test extension, flexion, adduction
- With the patient in the lateral decubitus position test abduction, IR, ER
Stability and special tests as directed by DDx:
- Assess sacroiliac joint stability
- FABER test
- FADIR test
- Squat test
- Trendelenburg test
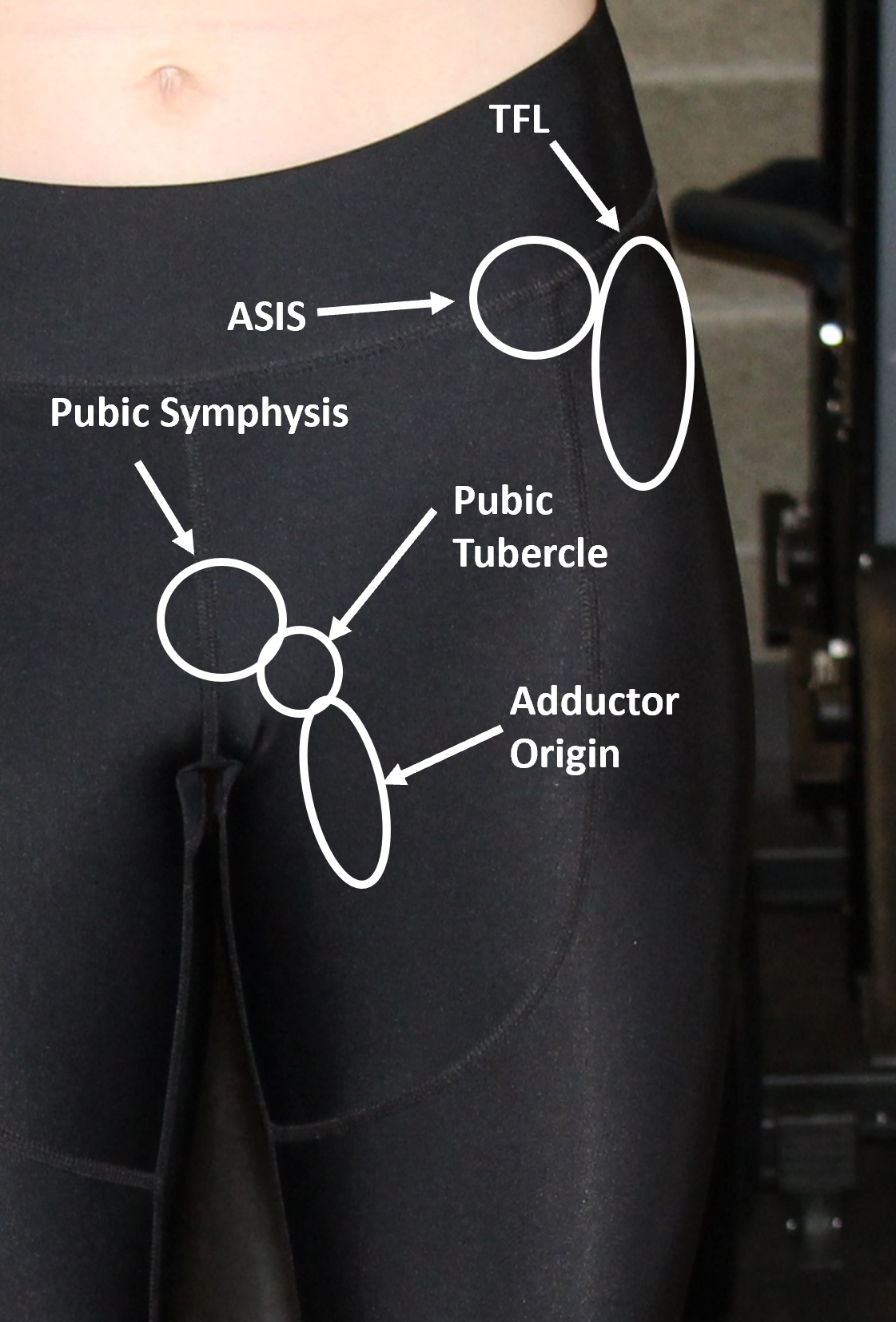
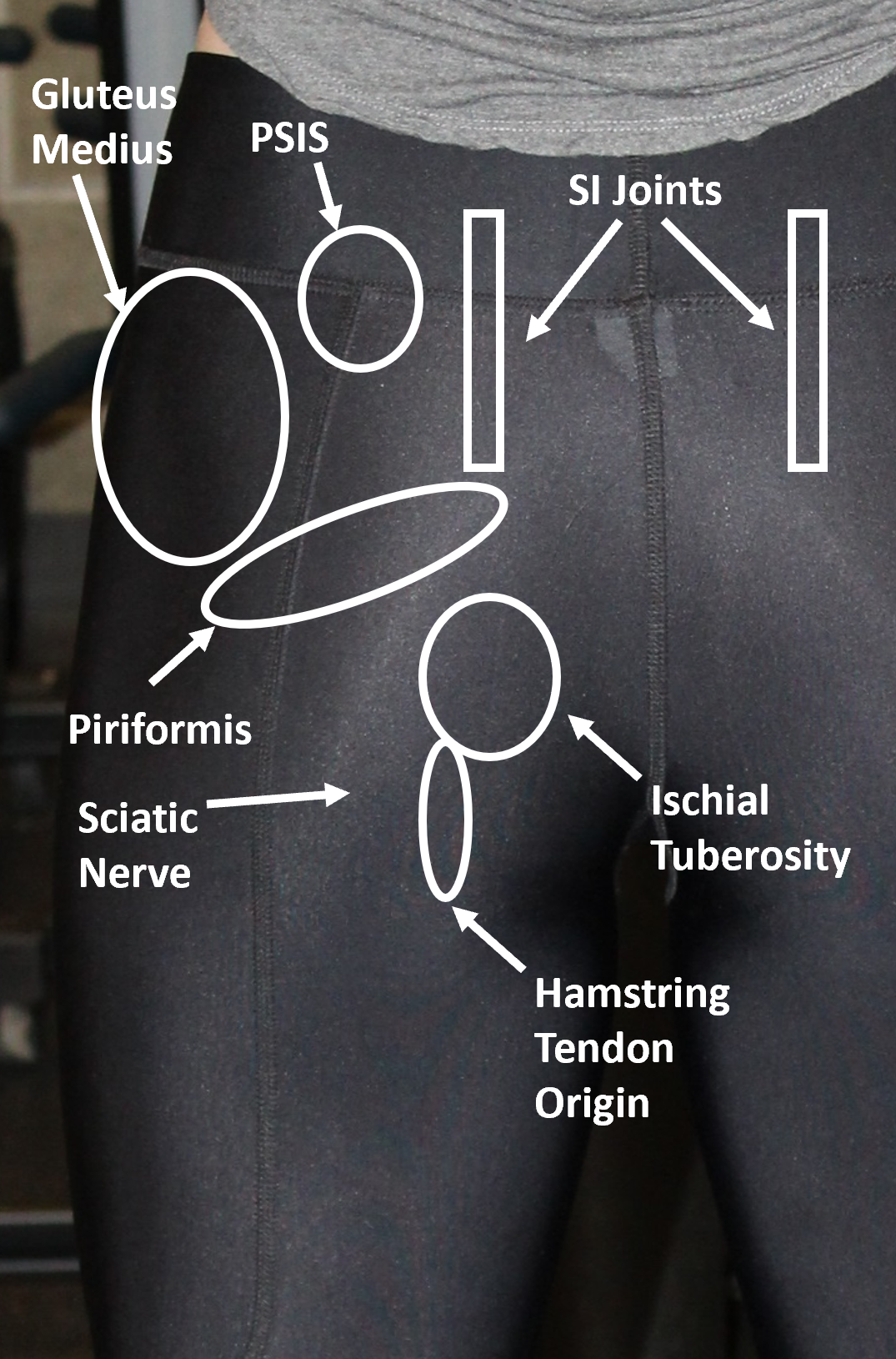
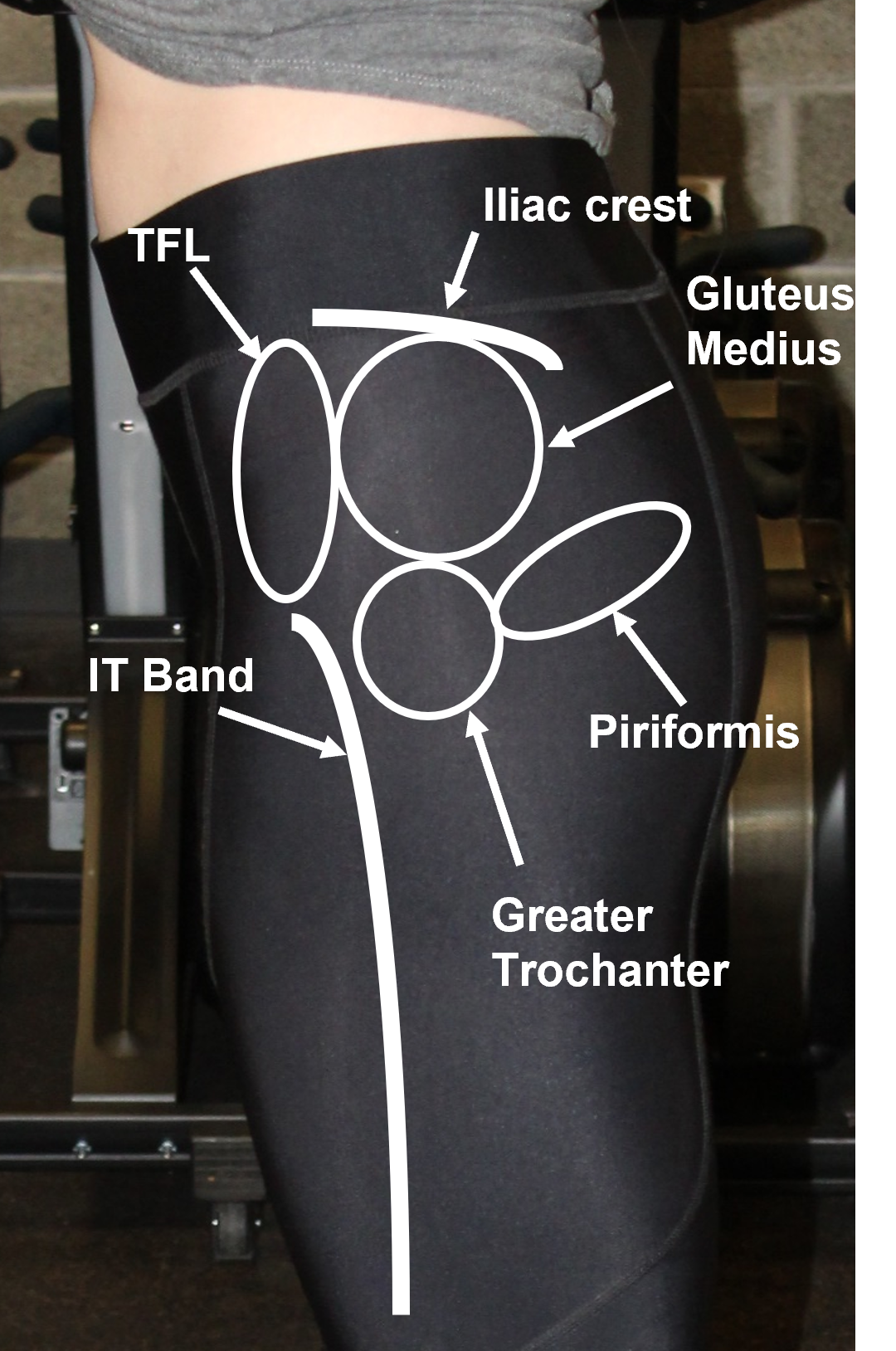
Key Landmarks & structures
Identify each of the anatomic landmarks.
 |
 |
 |
Inspection
Standing inspection should be performed for the anterior, lateral and posterior hip, noting swelling, erythema, ecchymoses, alignment and muscle bulk. Then, have the patient walk, observing for antalgia and functional range of motion.
Palpation
Palpate systematically, from the anterior to the lateral to the posterior structures of the hip above, noting any tenderness
Range of motion
Evaluate active and passive ROM. Normal ROM of the hip:
- Flexion (knee extended): 80-90 degrees
- Flexion (knee flexed): 110-120 degrees
- Extension: 10-20 degrees
- Adduction: 20-30 degrees
- Abduction: 30-50 degrees
- Internal rotation: 20-30 degrees
- External rotation: 40-50 degrees
Strength testing.
With the patient supine test:
- Extension
- Flexion
- Adduction
With the patient in the lateral decubitus position test:
- Abduction
- Internal rotation
- External rotation
STABILITY and SPECIAL TESTING
Assessing sacroiliac joint stability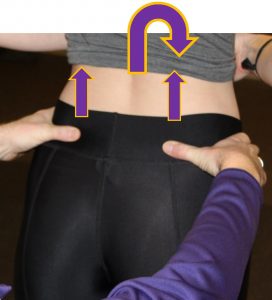
Instability of the SI joint is common and is typically caused by excessive gliding of the SI joints.
- Palpate the posterior superior iliac spines and ask the patient to bend forward
- Past 45 degrees of forward flexion, the PSIS should elevate
- With excess motion, the PSIS on the affected side will not move
FABER test
FABER is an acronym for Flexion, Abduction, External Rotation and tests for pathology of the ipsilateral hip and contralateral SI joint.

FADIR
FADIR is an acronym for Flexion, Adduction, Internal Rotation and tests for pathology of the ipsilateral hip joint.

Squat test
This test assesses pain with compression of intraarticular structures (e.g. labrum of the hip).

Trendelenburg test
This tests for weakness of the hip abductors (gluteus medius and minimus). Observe from behind the patient, as they place their hands on their hips on either side and stand on one leg and then the other. If the abductors are weak on the stance leg, the opposite side will drop. Those with significant hip abductor weakness may demonstrate Trendelenburg gait. As the patient bears weight on the affected side, the contralateral hemi-pelvis drops, causing a ‘lurch’ towards the affected side.
 |
 |