
MSK 1. C-Spine, Shoulder, Elbow, Wrist, Hand
Cervical Spine
C-spine Landmarks
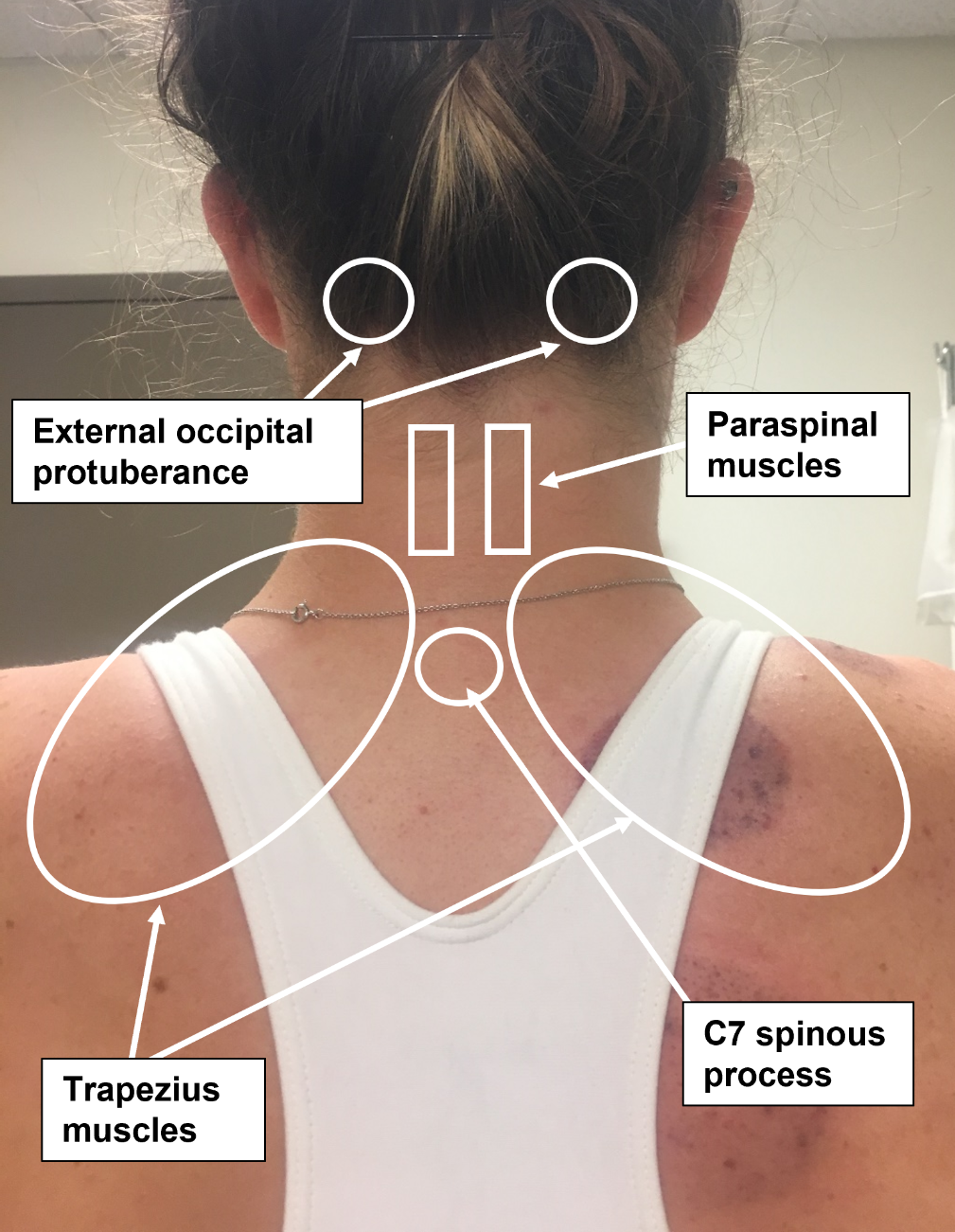 |
 |
Inspection
Inspect the neck and shoulders posteriorly, observing for symmetry of shoulder height and musculature, especially the trapezius.
Palpation
Palpate rom the occipital protuberance to C7, observing for pain or tenderness of the spinal column or paraspinous muscles.
Range of motion:
Assess active range of motion
- Flexion (normal is 80 to 90 degrees)
- Extension (normal is 70 degrees)
- Lateral rotation (normal is 90 degrees)
- Side bending (normal is 20 to 40 degrees)
Strength and neurovascular testing:
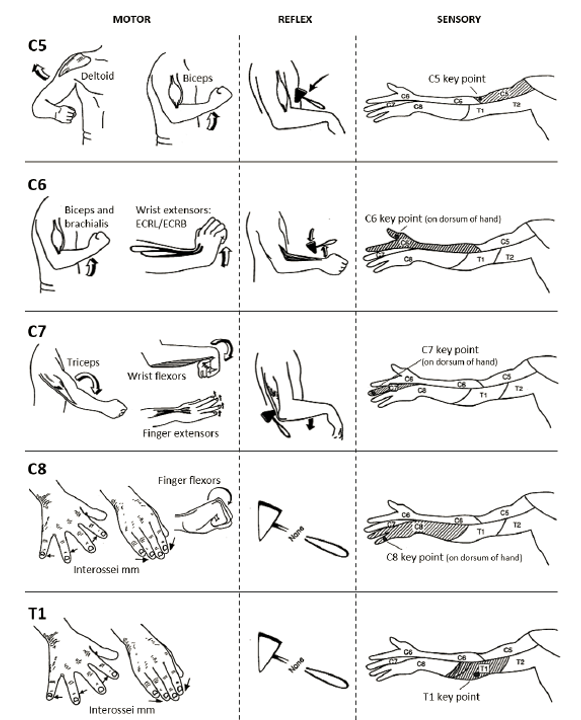
Cervical radiculopathy can affect one or more levels of the cervical spine, with characteristic patterns of weakness, numbness and reflex changes based on the levels that are affected.
To assess for compression of nerve roots or spinal cord, test
- Strength: Abduction of the shoulder, flexion and extension of the elbow, flexion and extension of the wrist, flexion, abduction and adduction of the fingers.
- Reflexes: Biceps, triceps, and brachioradialis
- Sensation: Key sensor points below

Spurling’s test. If you are concerned about cervical radiculopathy, perform Spurling’s Test The patient’s neck is extended and laterally rotated slightly, then an axial load is placed on the head by the examiner.Pain, numbness or tingling recreated in the upper extremity is considered a positive test and supports a diagnosis of a cervical radiculopathy
Benchmark Exam: Shoulder
Inspection
- Anterior, lateral and posterior shoulder
Palpation
- Palpate systematically, noting warmth, deformity, swelling and tenderness:
- Sternoclavicular joint
- Clavicle
- Acromioclavicular (AC) joint
- Biceps tendon in the bicipital groove
- Subacromial space and rotator cuff:
- Supraspinatus tendon
- Infraspinatus tendon
- Teres minor
- Subscapularis insertion
- Scapula
- Coracoid process
Range of motion
- Flexion, also called forward elevation
- Abduction
- Internal and external rotation
Strength Testing
- Flexion/forward elevation and extension
- Abduction and adduction
- Internal and external rotation
Stability and Special Tests (as directed by DDx)
- If you suspect rotator cuff dysfunction:
- Perform targeted strength testing of rotator cuff muscles:
- Empty can test
- Lift off test
- Assess for bursitis or impingement
- Neer test
- Hawkins test
- Perform targeted strength testing of rotator cuff muscles:
Shoulder Landmarks
| Right Shoulder– Anterior view | Right Shoulder– Lateral view | Right Shoulder– Posterior view |
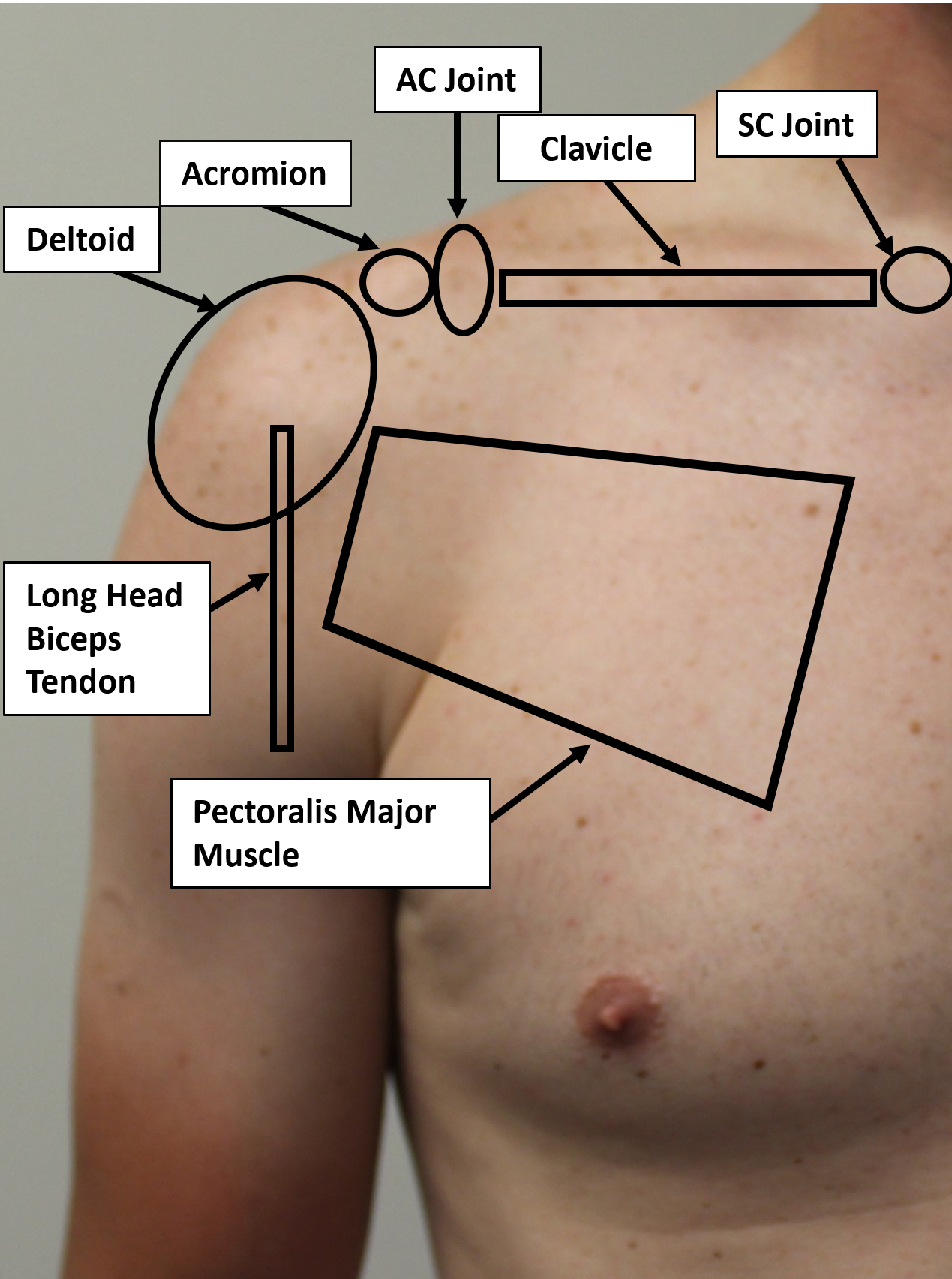 |
 |
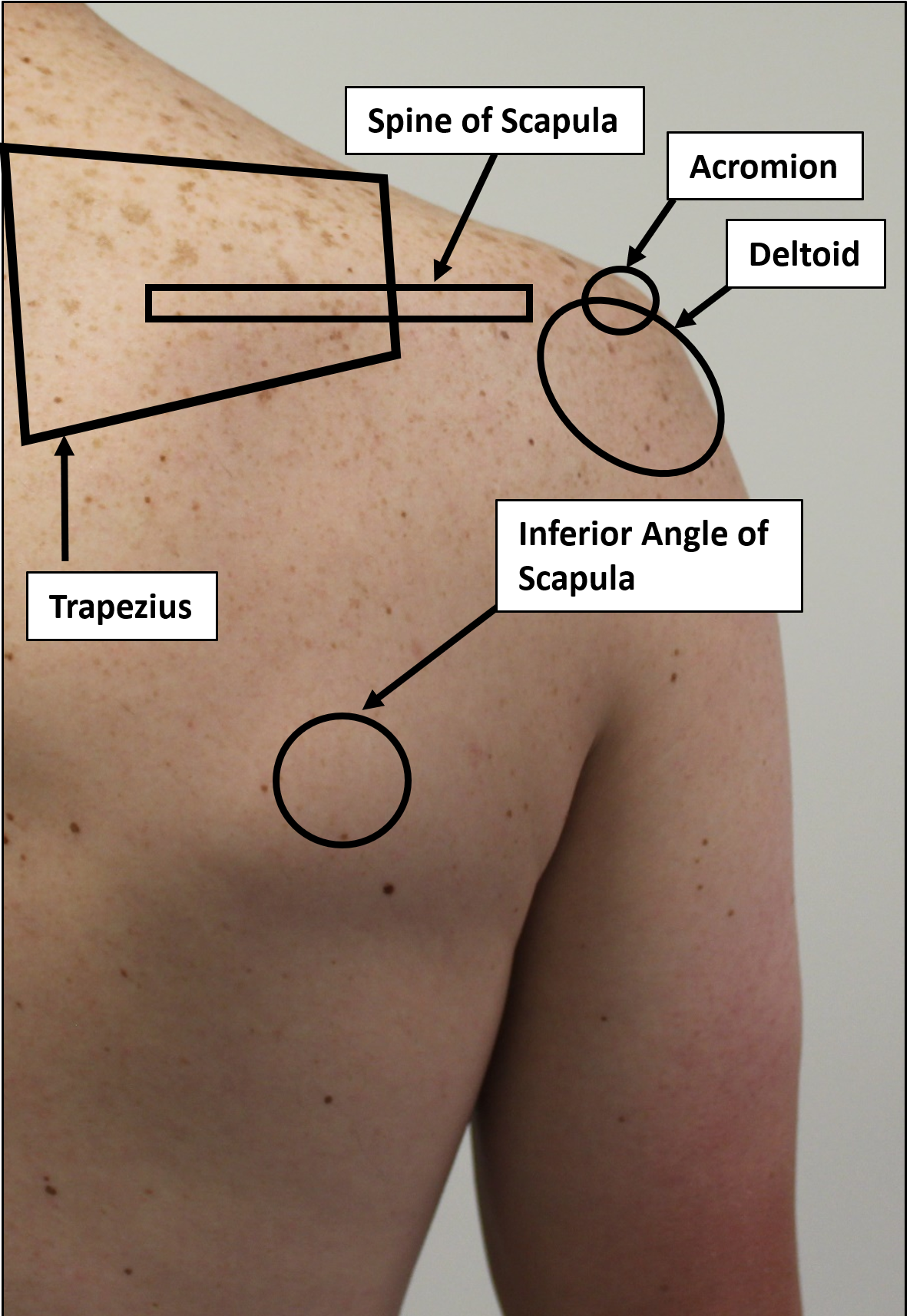 |
Inspection
Assess for symmetry, swelling, trauma or erythema of the anterior, lateral and posterior shoulder.
Palpation
Palpate the shoulder systematically, starting with the sternoclavicular joint and moving systematically, from anterior to lateral to posterior.
-
- Sternoclavicular joint
- Clavicle
- Acromioclavicular (AC) joint
- Biceps tendon in the bicipital groove
- Coracoid process is the origin of the short head of the biceps
- Subacromial space and rotator cuff:
- supraspinatus tendon lies just below the anterior lateral acromion
- infraspinatus tendon lies just below posterolateral acromion
- teres minor lies just inferior to the infraspinatus
- subscapularis insertion lies just lateral to coracoid at the anterior shoulder
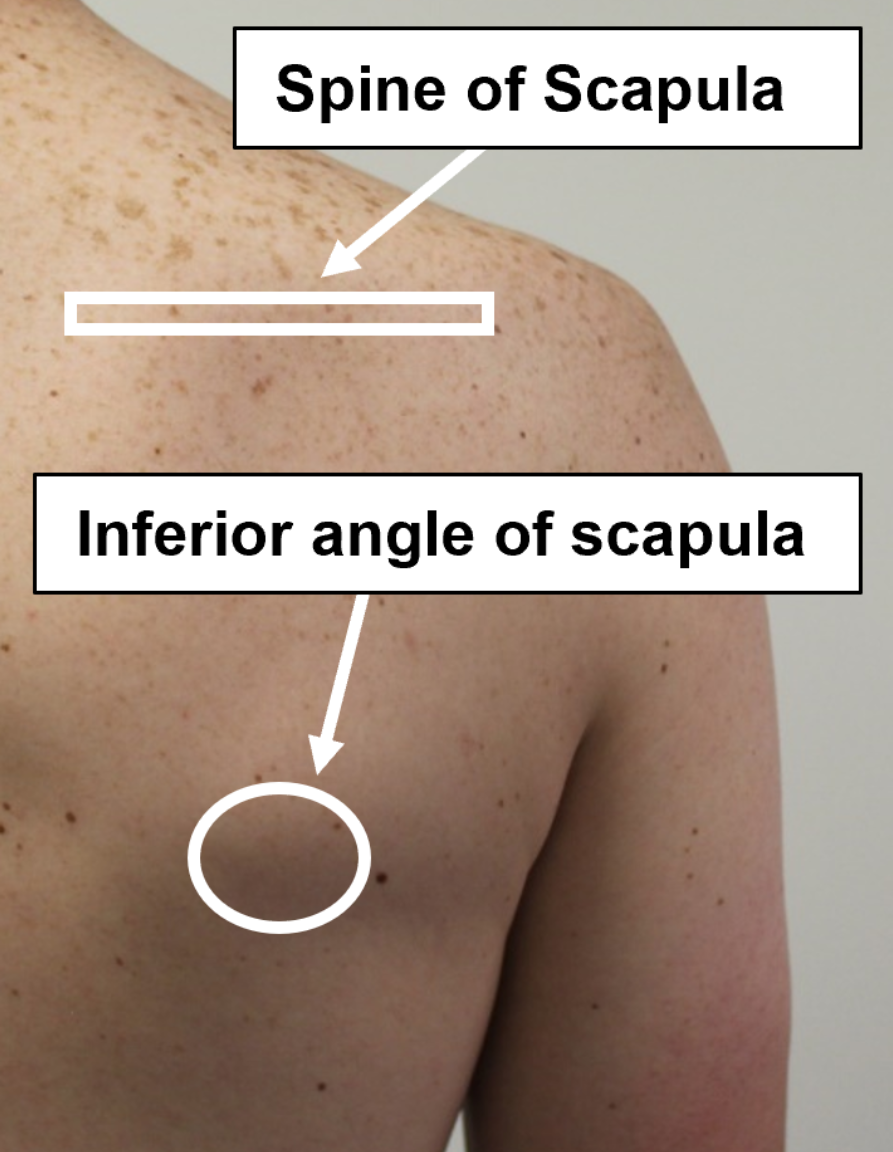
- Scapula:
- spine of the scapula is the origin of the infraspinatus
Range of motion
Assess active and passive ROM in each plane: flexion, abduction, internal and external rotation. If range of motion is limited, note whether it is limited by pain or “true” restriction. Adhesive capsulitis, glenohumeral osteoarthritis and dislocation limit or cause pain with both active and passive ROM. Injury of muscles or ligaments such as rotator cuff tendonitis affect active more than passive ROM. Increased ROM of the shoulder suggests ligamentous laxity or prior dislocations.
You can also assess the shoulder with simple functional tests.
- Internal rotation and adduction: Ask your patient to reach up behind the back to touch the highest point on the spine that they can. This tests internal rotation and adduction. Normal shoulder ROM is to reach up to T10 (count down from T7 at the lower border of the scapula or up from L4 at the level of the iliac crest).
- External rotation and abduction: Ask your patient to reach as far down behind their head as they can to touch the spine. This tests external rotation and abduction. Normal shoulder ROM is to reach down to T1 (below C7, the prominent bump at the base of the neck)
Strength testing
With your patient seated, test strength of shoulder flexion, extension, abduction, adduction, internal and external rotation, grading each movement on the 0-5 scale. If you suspect long thoracic nerve injury, you can test subscapularis strength by asking your patient to perform a ‘mini-push up’ against the wall and observing for scapular winging.
Stability & special testing
Targeted testing of rotator cuff muscles
Rotator cuff disorders include tendinitis, tear, subacromial bursitis, and impingement syndromes. Different examiners prefer different special tests when rotator cuff pathology is suspected. You will practice those with the strongest evidence base in FCM.
The rotator cuff is made up of the 4 ‘SITS’ muscles. Targeted strength testing of these muscles may reveal pain, which suggests tendinitis, or weakness, which supports a rotator cuff tear.
- Supraspinatus: abduction from 0 to 90 degrees
- Infraspinatus: external rotation
- Teres Minor: external rotation
- Subscapularis: internal rotation
Lift-off test

The lift-off test assesses the subscapularis muscle.
With the shoulder fully internally rotated, the patient attempts to lift their hand away from the back as the examiner applies pressure to the forearm.
Pain with this maneuver supports tendinitis while weakness suggests a subscapularis tear.
Empty can test
 The empty can test isolates the supraspinatus muscle.The shoulder is held in 80 degrees of flexion, 45 degrees of abduction and full internal rotation as if emptying a can of soda. Downward pressure is placed on the arm as the patient resists.
The empty can test isolates the supraspinatus muscle.The shoulder is held in 80 degrees of flexion, 45 degrees of abduction and full internal rotation as if emptying a can of soda. Downward pressure is placed on the arm as the patient resists.
Pain with this maneuver supports tendinitis while weakness suggests a supraspinatus tear
Special tests for rotator cuff impingement
The rotator cuff tendons occupy a narrow space between the acromion and the head of the humerus. Impingement, or pinching, of the tendons between these two structures is a common cause of shoulder pain. Pain with the Neer or Hawkins/Kennedy test, both of which narrow the space even further, support a diagnosis of rotator cuff impingement, which is usually caused by swelling of the tendons or bursa.

Elbow
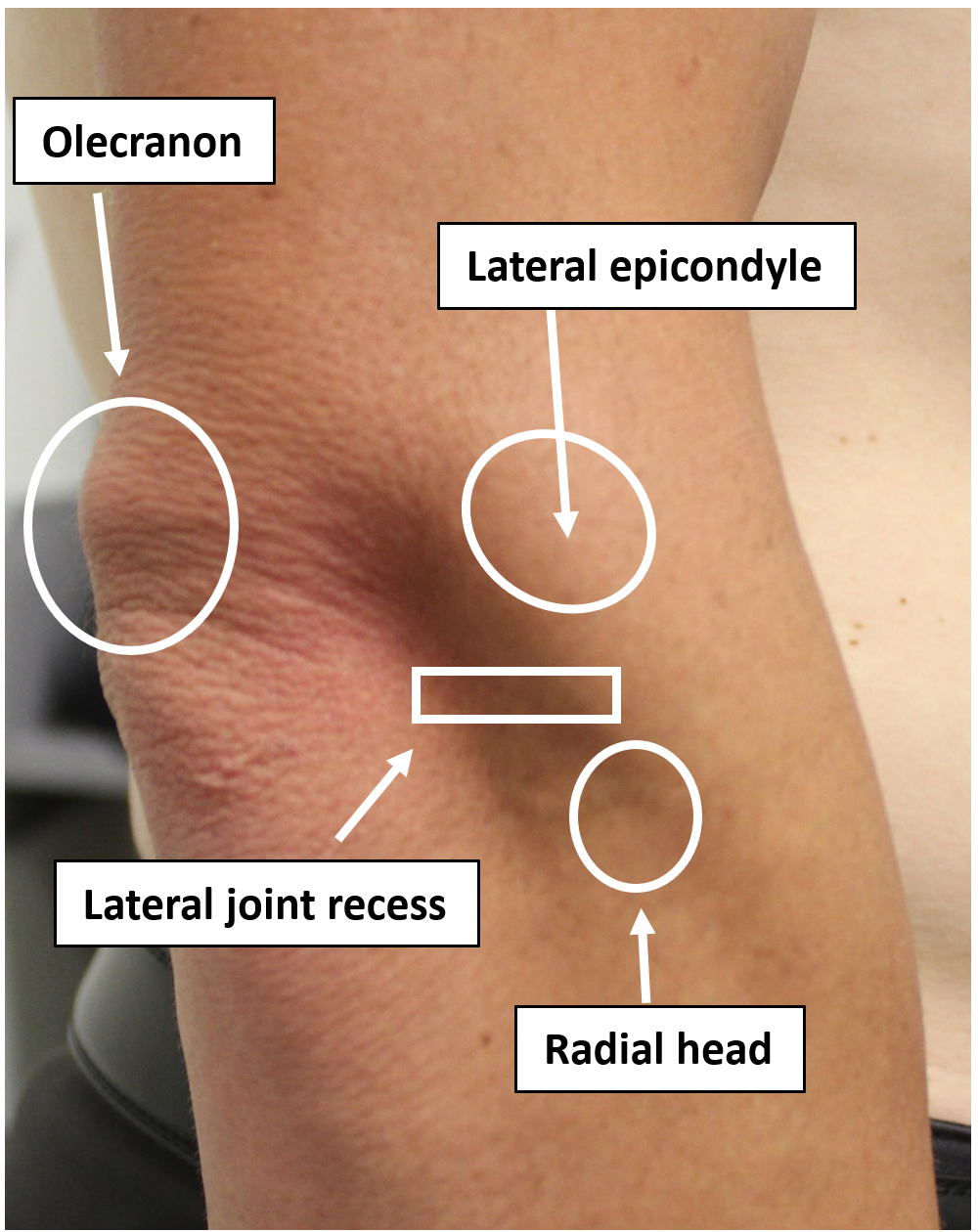
Elbow Landmarks
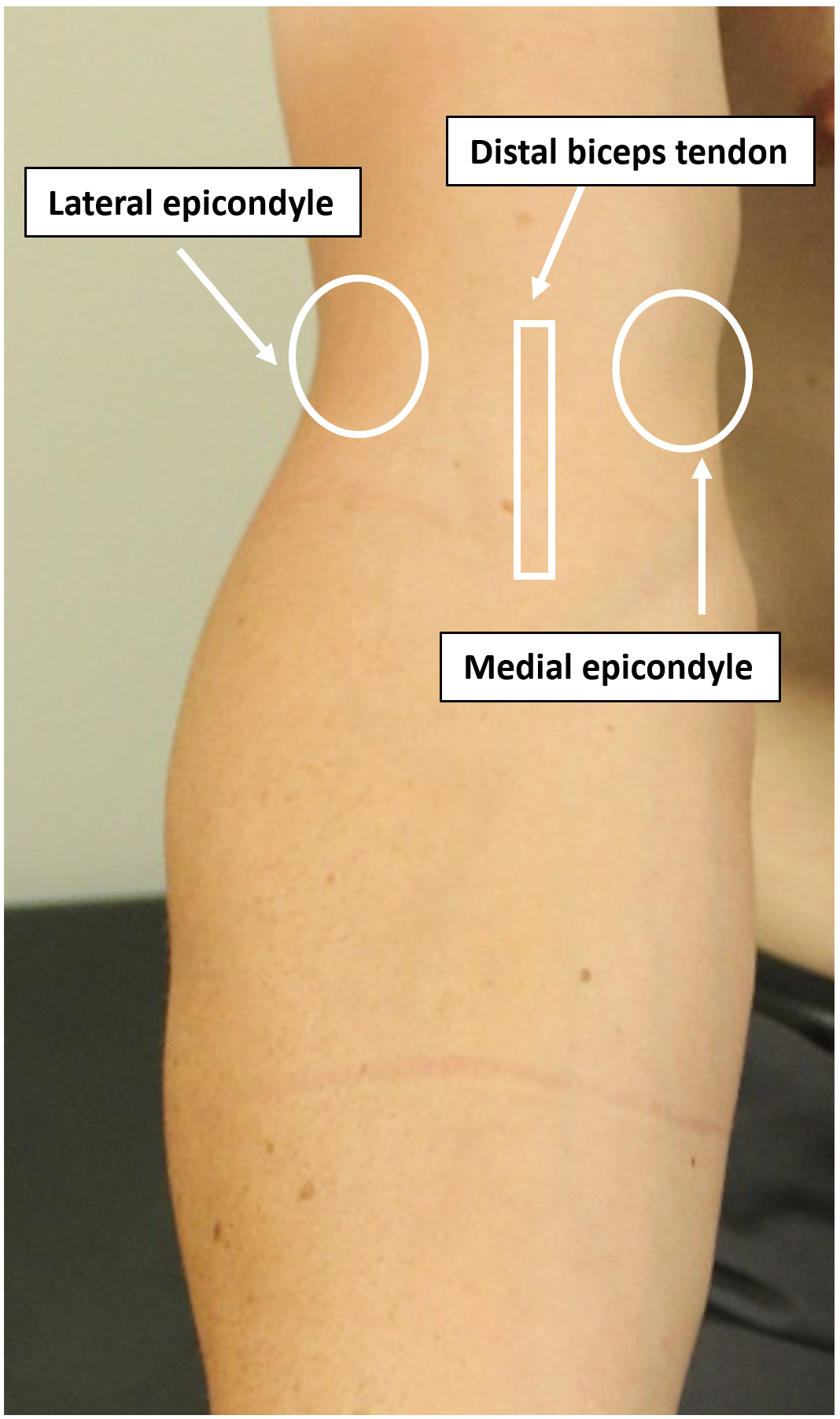 |
 |
 |
Inspect: Dorsal, lateral and ventral elbow
Palpate: affected area, observing for tenderness and swelling.
Range of motion: Flexion (140°), extension (10°), supination (80°) , pronation (80°)
Strength testing: Extension, flexion, supination, pronation
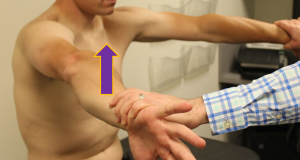
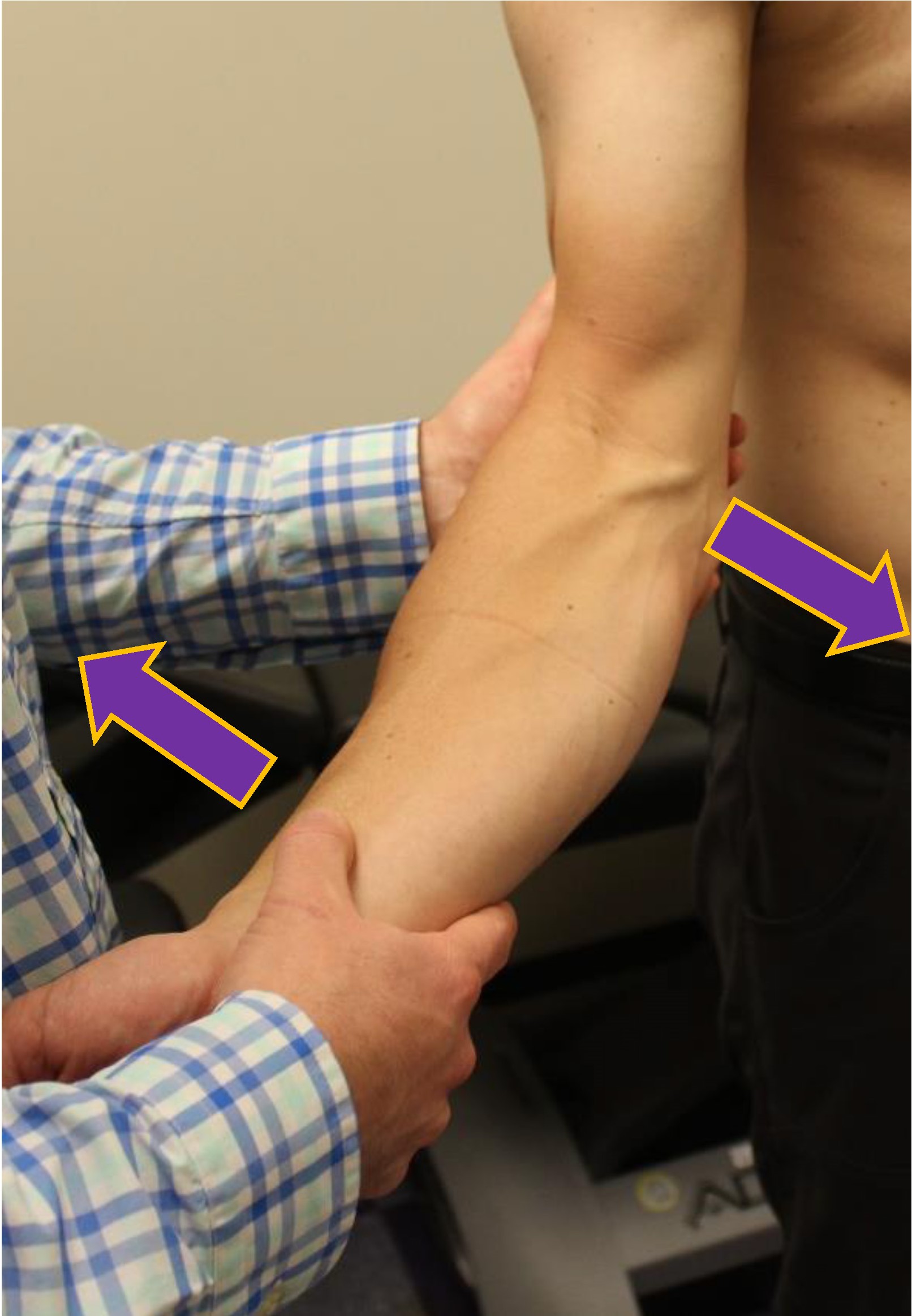 Stability testing of the ulnar and radial collateral ligaments is performed with the patient seated and the elbow extended to both zero and thirty degrees. Make note of pain or laxity with valgus or varus stress. Compare to the asymptomatic side.
Stability testing of the ulnar and radial collateral ligaments is performed with the patient seated and the elbow extended to both zero and thirty degrees. Make note of pain or laxity with valgus or varus stress. Compare to the asymptomatic side.
-
-
-
- Ulnar (medial) collateral ligament: Place valgus stress on the elbow by applying pressure to the lateral elbow with one of your hands and with the other hand, pushing the patient’s forearm laterally (image at left)
- Radial (lateral) collateral ligament: Place varus stress on the elbow by applying pressure to the medial elbow with one hand on the medial elbow while pushing the patient’s forearm medially
-
-
Wrist & Hand
Landmarks
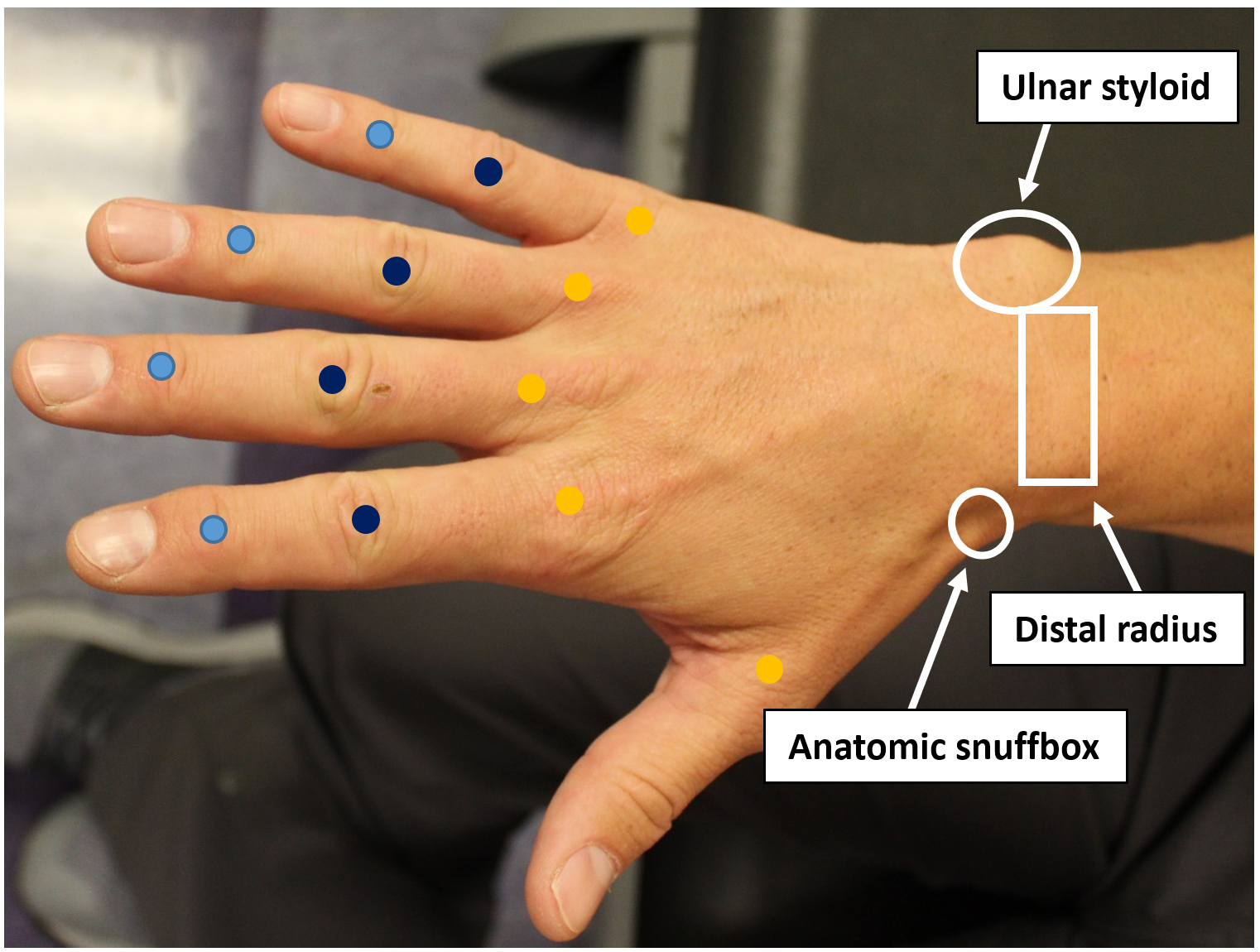
| Right wrist and hand – Dorsal view | Right wrist and hand– Palmar view |
 |
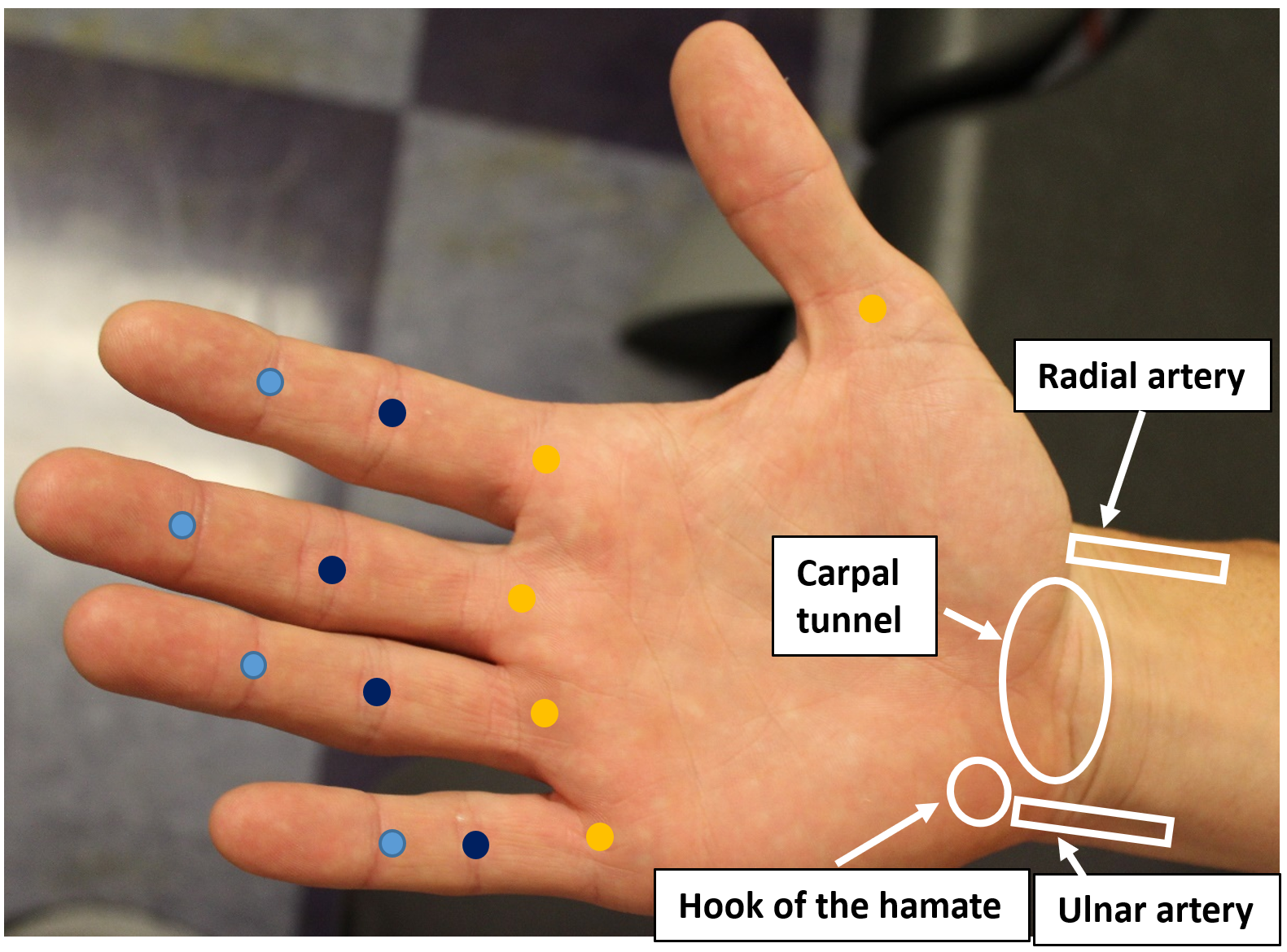 |
Inspect and palpate the dorsal and palmer wrist and hand, focusing on the symptomatic area.
Range of motion of the wrist:
- Flexion: 75°
- Extension: 75°
- Ulnar deviation: 40°
- Radial deviation: 20°
Range of motion of the hand:
- DIP/PIP Flexion: 90 °
- DIP/PIP Extension: 0°
- MCP Flexion: 90°
- MCP Extension: 5 to -10 °
Stability and Special tests
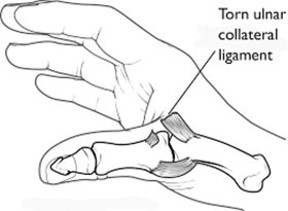 Stability testing of the ulnar collateral ligament of the thumb.
Stability testing of the ulnar collateral ligament of the thumb.
Each metacarpophalangeal and interphalangeal joint has both ulnar and radial collateral ligaments. The UCL of the thumb is commonly injured (skier’s or gamekeeper’s thumb) which can lead to significant morbidity if not treated properly. To assess UCL stability, hold the thumb flexed 45 degrees towards the palm and apply valgus stress to the proximal phalanx. Compare the degree of laxity and firmness of the endpoint to the opposite side.

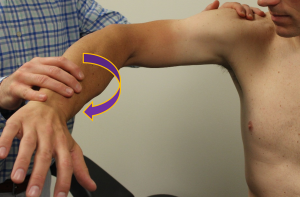
Finkelstein’s test for DeQuervain’s tendinitis
The thumb is held in patient’s palm and the examiner moves the hand and wrist into ulnar deviation, which stresses the first dorsal compartment of the wrist.
Pain with ulnar deviation is considered a positive test
Tests for Carpal Tunnel Syndrome
 Phalen’s test
Phalen’s test
- Hands are pressed together forcing both wrists into flexion and compressing the carpal tunnel
- Pain, numbness, tingling the distribution of the median nerve indicates a positive test for carpal tunnel syndrome
Tinel’s test
- Examiner uses the thumb to compress the carpal tunnel
- An alternative method is to tap the middle finger repeatedly over the carpal tunnel
- Pain, numbness, tingling the distribution of the median nerve indicates a positive test for carpal tunnel syndrome
Knowledge check
After reviewing this chapter, what connections are you making with the anatomy and conditions that you have learned about in the MSK block? What anatomy and exam findings are still confusing?