
9 Lab Week 9: Hypothalamus, Limbic System, and Thalamus Review
Learning Objectives
1. Hypothalamus
Describe the location of the hypothalamus and its nearest neighbors.
List the major functions of the hypothalamus, and relate these to its connections.
Distinguish between the neural and non-neural inputs, and neural and neuro-endocrine outputs, of the hypothalamus.
Describe the output of the hypothalamus involved in controlling a. the pituitary and b. the autonomic system.
Describe Horner’s syndrome and possible lesion sites that produce it.
2. Limbic System
List the structures that comprise the limbic lobe.
Describe the location of the hippocampus and its major connections, and summarize its functions.
Describe the location of the amygdala and its major connections, and summarize its function.
Locate in gross brains, MRIs and sections: the limbic lobe, hippocampus, hypothalamus, mammillary bodies, fornix, amygdala.
Describe the consequences of bilateral temporal lobectomy (Kluver-Bucy syndrome).
3. Thalamus
Describe the relations of the thalamus and internal capsule.
List the major inputs and cortical connections of the major thalamic nuclei.
This last lab explores the hypothalamus and limbic system, which are strongly interconnected and work together to ensure the survival of the individual and the species, by regulating homeostasis and drive-related behavior. We include an exercise on the thalamus for review.
Hypothalamus
The hypothalamus is part of the diencephalon. It is tiny but packs a lot of punch functionally, serving to regulate the autonomic system and pituitary gland. Because it regulates such functions as temperature, blood pressure, metabolism, water balance, circadian rhythms, and reproductive, defensive and emotional behaviors, hypothalamic tumors or lesions can manifest in an amazing variety of symptoms, e.g. mood disorder, temperature regulation problems, dysphagia, memory problems, among others.
A helpful mnemonic is “HEAL”
Hypothalamus functions to maintain: Homeostasis by regulating the Endocrine, Autonomic and Limbic systems.
Anatomy
The hypothalamus forms the floor and lower part of the walls of the third ventricle. In a ventral view of the brain it is diamond-shaped: the optic chiasm and tracts lie anteriorly and the cerebral peduncles lie posteriorly. The only parts of the hypothalamus seen in a ventral view are the mammillary bodies, the infundibulum (from which the pituitary gland is usually severed), and the floor of the hypothalamus (tuber cinereum). The swelling at the base of the infundibulum is the median eminence. All of these are exposed to CSF in the subarachnoid space.
Neighboring structures are best appreciated in sagittal, coronal or horizontal views. The basal forebrain lies laterally but there is no obvious lateral boundary in gross specimens. Superiorly, the hypothalamic sulcus separates the hypothalamus from the thalamus. The posterior border is an arbitrary line drawn vertically upwards from the posterior aspect of the mammillary bodies.
Make sure you can recognize the boundaries of the hypothalamus in the following images.
Nuclei
The hypothalamus is a collection of about a dozen nuclei. The ones we ask you to know are the
- suprachiasmatic nucleus: lies dorsal to the optic chiasm, gets a major input from the retina, and is important in circadian rhythms
- supraoptic and paraventricular nuclei: secrete oxytocin and antidiuretic (ADH) hormones. Oxytocin is important in generating uterine contractions during labor, ADH conserves water at the level of the kidneys. Alcohol inhibits ADH and hence causes urination.
- mammillary nuclei: as part of Papez’ circuit which loops through the hippocampus, the mammillary nuclei are involved in consolidation of memory. Conditions like thiamine deficiency affect these nuclei causing memory deficits as part of Korsakoff’s syndrome.
The anterior and posterior nuclei are involved in thermoregulation, the ventromedial nucleus is important in hunger regulation and satiety – several drugs are being developed to target these nuclei in an attempt to control obesity.
In the frontal plane, the hypothalamus is often divided into periventricular, medial and lateral zones. The medial and lateral zones are divided by the fornix as it arches down to terminate in the mammillary bodies.
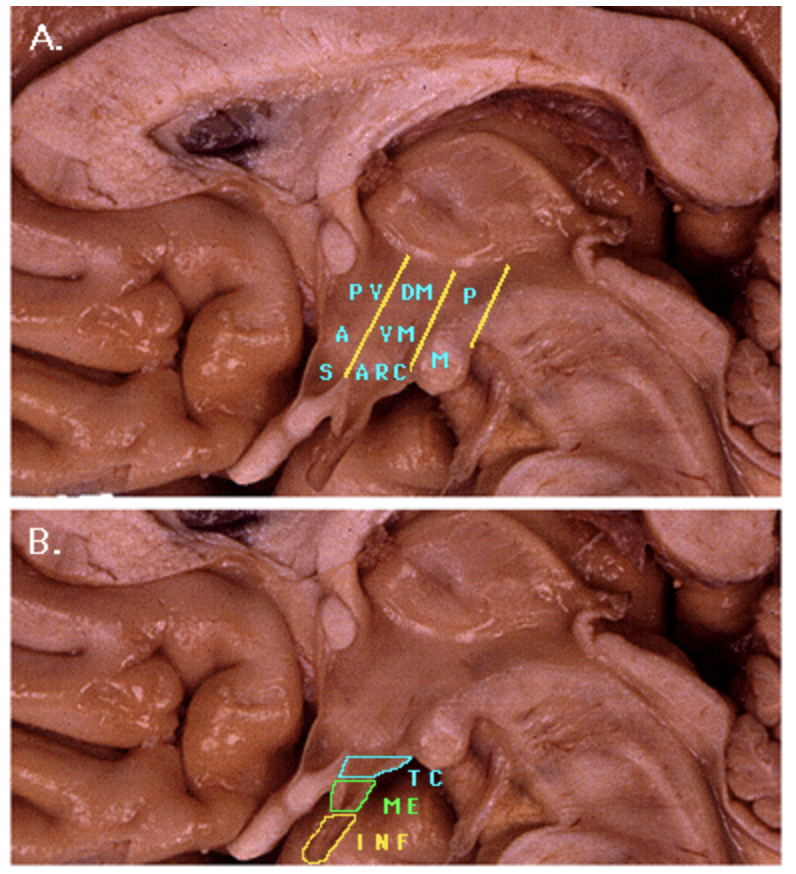
In a sagittal view, the anterior-posterior regions of the hypothalamus can be appreciated. In A below, the anterior, middle (AKA tuberal) and posterior regions can be seen each wth the locations of their most important nuclei shown. S suprachiasmatic and supraoptic nuclei, A anterior hypothalamic nucleus, PV paraventricular nucleus, ARC arcuate nucleus, VM ventromedial nucleus, DM dorsomedial nucleus, P posterior hypothalamic nucleus and M mammillary nuclei.
In B, details of the base of the hypothalamus are shown: INF infundibulum, ME median eminence, and TC tuber cinereum (ie the floor of the hypothalamus excluding the mammillary bodies)
Connections
As noted above, there are many nuclei in the hypothalamus, each with specific inputs and outputs. A unique aspect of hypothalamic “connectivity” is that some inputs are directly sensed by neurons in the hypothalamus. For example, some hypothalamic neurons function as sensors of osmolarity.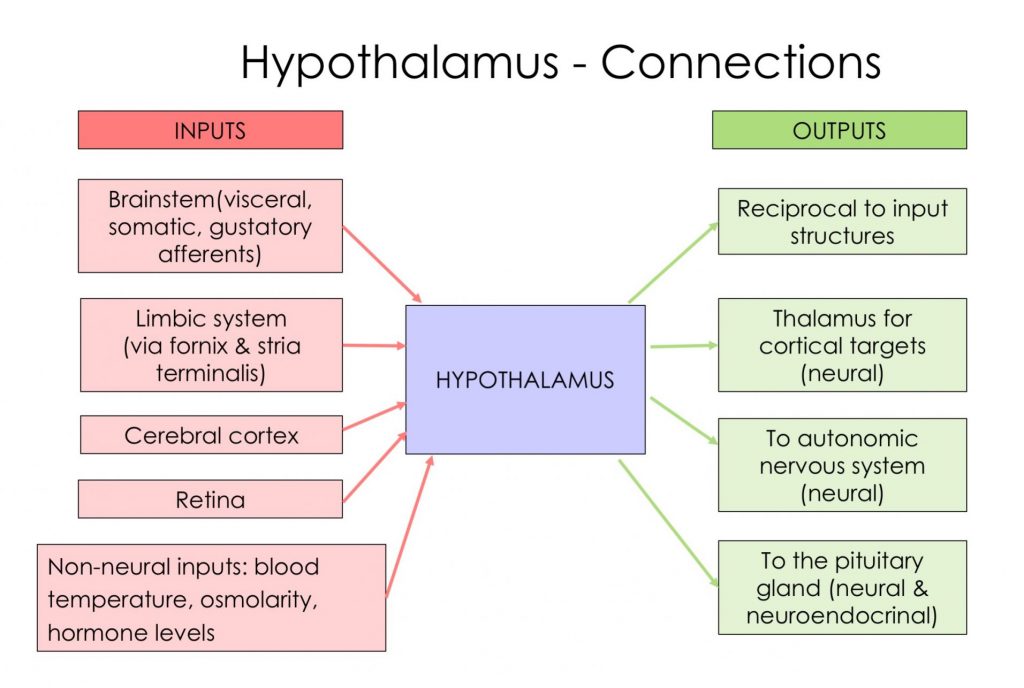
Inputs:
- from olfactory areas, cortex and limbic structures
- via fornix from hippocampus
- via stria terminalis and other paths from amygdala
- dorsal longitudinal fasciculus (DLF) from brainstem (e.g. taste and somatic afferents; solitary nucleus visceral afferents)
- optic tract from retina (for circadian rhythm entrainment)
- non-neural inputs (blood temp, osmolarity, hormone levels, etc)- a subset of hypothalamic neurons directly sense these
The hypothalamus is also unique in that some of its outputs are in the form of neurohormonal (neuroendocrinal) release into the circulation for transport to distant targets. This type of communication is thus on a different time scale than synaptic communication.
Some hypothalamic nuclei secrete releasing or inhibiting hormones into the blood vessels in the median eminence. These vessels travel to capillary beds in the anterior pituitary (hypophyseal portal system) and regulate secretion of hormones from the pituitary cells there. The hypothalamus thus regulates the “master gland” of the body. Two hypothalamic nuclei (supraoptic and paraventricular nuclei) have axons that form the infundibular stalk and their terminals in the posterior pituitary release the hormones oxytocin and ADH (anti-diuretic hormone or vasopressin) into the systemic circulation, which delivers them to receptors in the kidney and uterus.
Many of the hypothalamic nuclei make regular synaptic contact with nuclei throughout the brain and cord, through which the hypothalamus regulates the autonomic system and influences activity in the limbic system. It is noteworthy that a single hypothalamic nucleus may have neuron populations with quite different functions, eg. some neurons in the paraventricular nucleus release neurohormones, while others have axons that contribute to descending tracts that synapse on neurons regulating autonomic function.
Outputs:
- reciprocal neural output to same places that send input (except retina): to cortex, limbic structures, brainstem, and cord.
- to pituitary via hypothalamo-hypophyseal tract (fancy name for axons of SO and PV nuclei axons in the infundibulum) and via the hypophyseal portal system (hypophysis is another term for pituitary, and this system refers to the neurohormonal outputs that control the anterior pituitary).
- mammillothalamic tract to anterior nucleus of thalamus.
- descending projections to brainstem and spinal cord via DLF and hypothalamospinal tract.
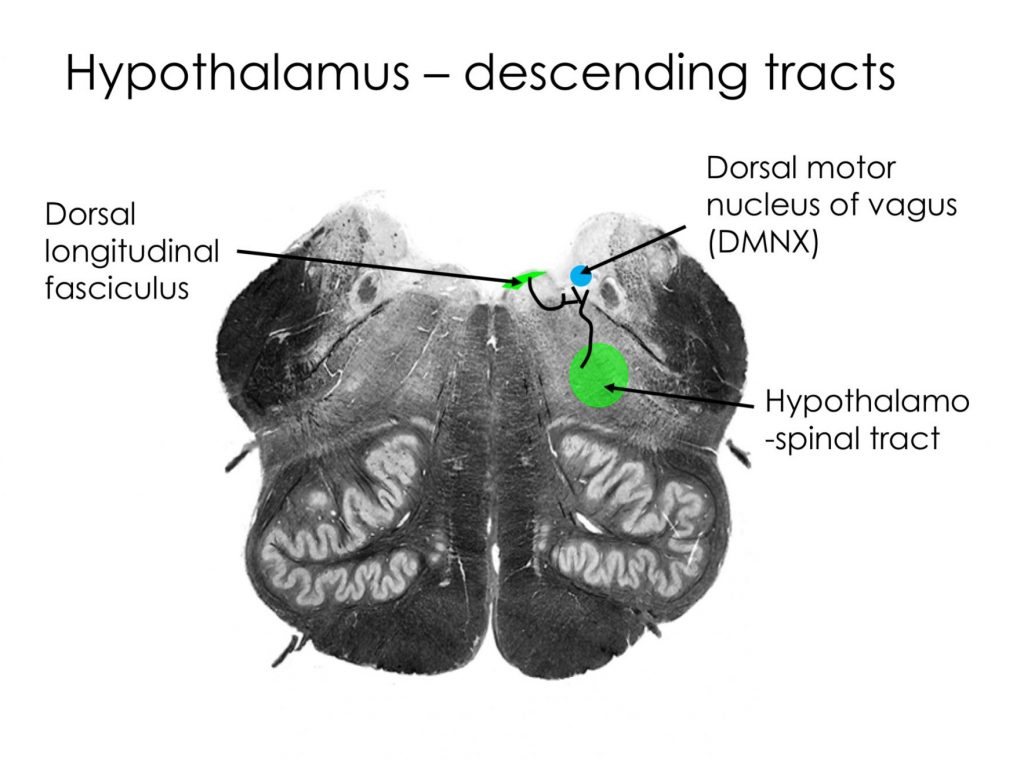
Descending Connections From Hypothalamus to Brainstem and Spinal Cord: Major Influence on Autonomic Outflow
The hypothalamus is the “head ganglion” of the autonomic system. It receives input from viscera (via pathways from the visceral afferents in cranial nerves and via circulating hormones etc) and projects directly to parasympathetic and sympathetic nuclei, and indirectly to them, relaying through other brainstem nuclei important in visceral function. The two major systems descending from the hypothalamus to the autonomic efferents are ipsilateral: the dorsal longitudinal fasciculus to the brainstem, and a tract we can call the “hypothalamo-spinal tract” to the spinal cord (it runs in the dorsolateral tegmentum, and subsequently in the lateral white matter of the cord). Locations of descending fibers are shown below.
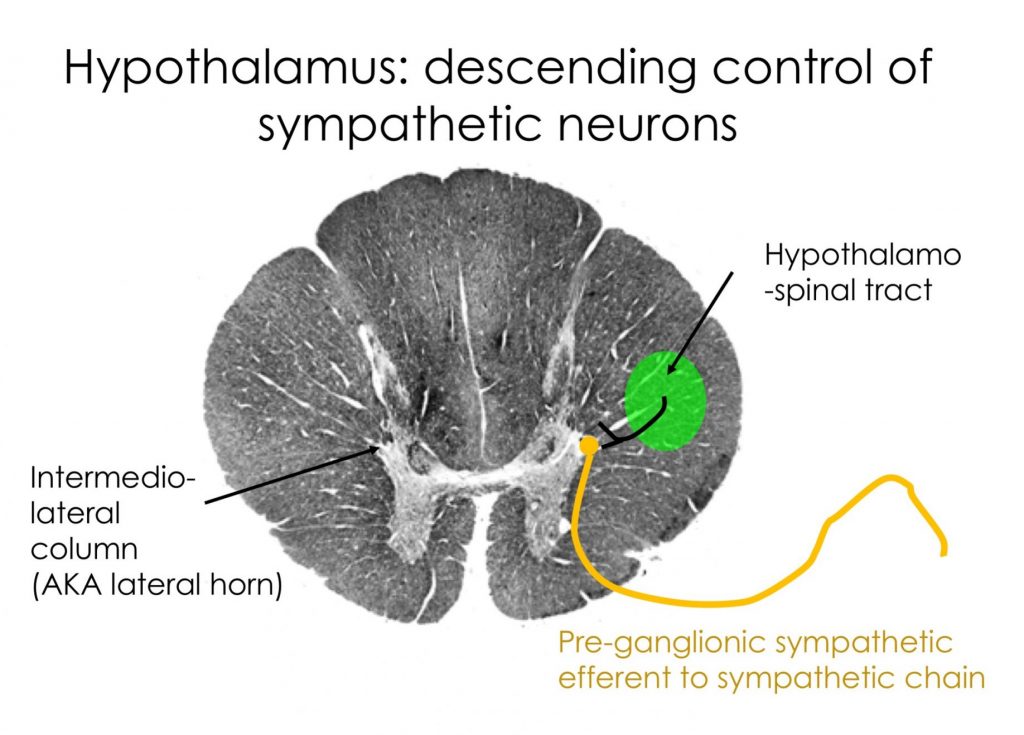
Horner’s syndrome is an example of disruption to the sympathetic innervation to the head somewhere along the long pathway from the hypothalamus (in the CNS) to the target structures in the periphery (specifically the dilator of the pupil, the smooth muscle in the upper eyelid, sweat glands in the face).
The syndrome presents on one side of the face (ipsilateral to the damage):
- ptosis (drooping eyelid)
- miosis (constricted pupil)
- anhydrosis (loss of sweating), vasodilation
The syndrome has limited utility in localizing a lesion, as the pathway is so long and passes through both the CNS and PNS. It can result for example from a lesion to
- the hypothalamus or hypothalamospinal fibers in the lateral tegmentum of the brainstem or lateral white matter of the cord
- the lateral horn neurons in T1-T2 cord segments
- the pre-ganglionic sympathetic axons or sympathetic chain neurons (e.g. a tumor in the apex of the lung may disrupt sympathetic chain ganglia)
- postganglionic sympathetic axons en route to head in the carotid plexus (sympathetic axons travel to the head on the surface of the carotid arterial system)
If you review the clinical lab material, you will note that lateral medullary syndrome presents with ipsilateral Horner’s syndrome-now you can understand why.
Limbic System
The limbic system is the collection of cortical and subcortical structures located along the medial edge of the cerebral hemispheres. (Limbus, Latin for margin or border). Collectively, limbic structures play a role in emotions and emotional behaviors, and in learning and memory. The term limbic system has limited usefulness: as we learn more it seems that the limbic system may be comprised of several subsystems, with distinct connections and functions. Sometimes, the term medial temporal lobe is used to collectively refer to the hippocampus, amygdala, and overlying cortex. Recall that these structures all lie on the tentorium very close to the tentorial notch, and may herniate through that opening when supratentorial pressure rises, for example, as a result of a bleed, tumor or swelling in the cortex.
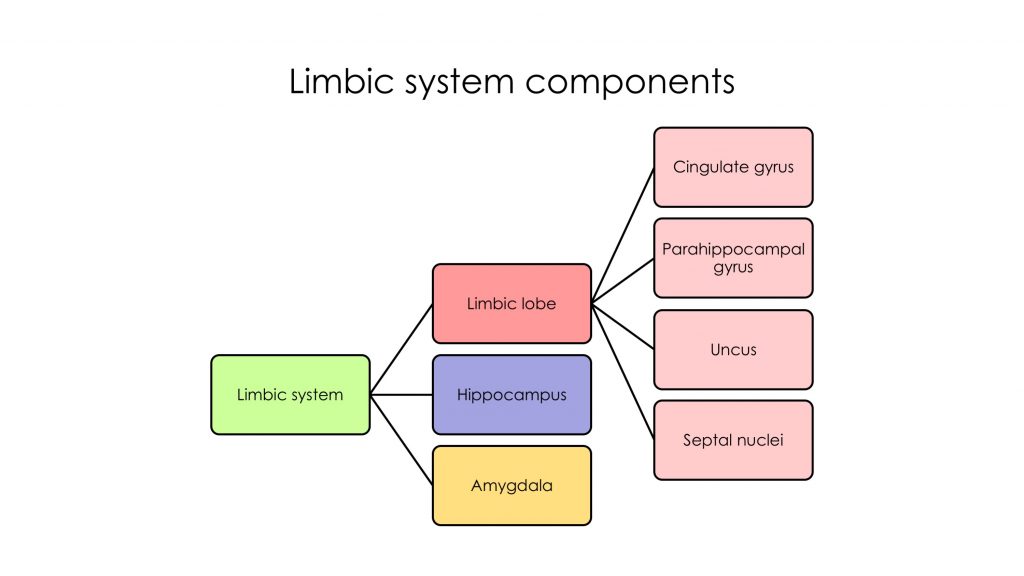
There is a lack of agreement about which structures make up the limbic system, and you may find variations in descriptions of components among your resources. We consider here just the limbic lobe (consisting of subcallosal, cingulate and parahippocampal gyri and the uncus), the amygdala and the hippocampus. The limbic lobe forms a C-shape, and the hippocampus and its output fibers (the fornix), and the amygdala and its output tract (the stria terminalis, not easily seen in our materials) also form C-shaped structures nested inside the limbic lobe.
Recall that the hippocampus is 3-layered cortex in an elaborate swirling pattern often visible to the naked eye; it lies deep to the parahippocampal gyrus and forms the medial wall of the inferior horn of the lateral ventricle. The amygdala, a more or less spherical nucleus, lies deep to the uncus, and is largely anterior to the inferior horn of the lateral ventricle.
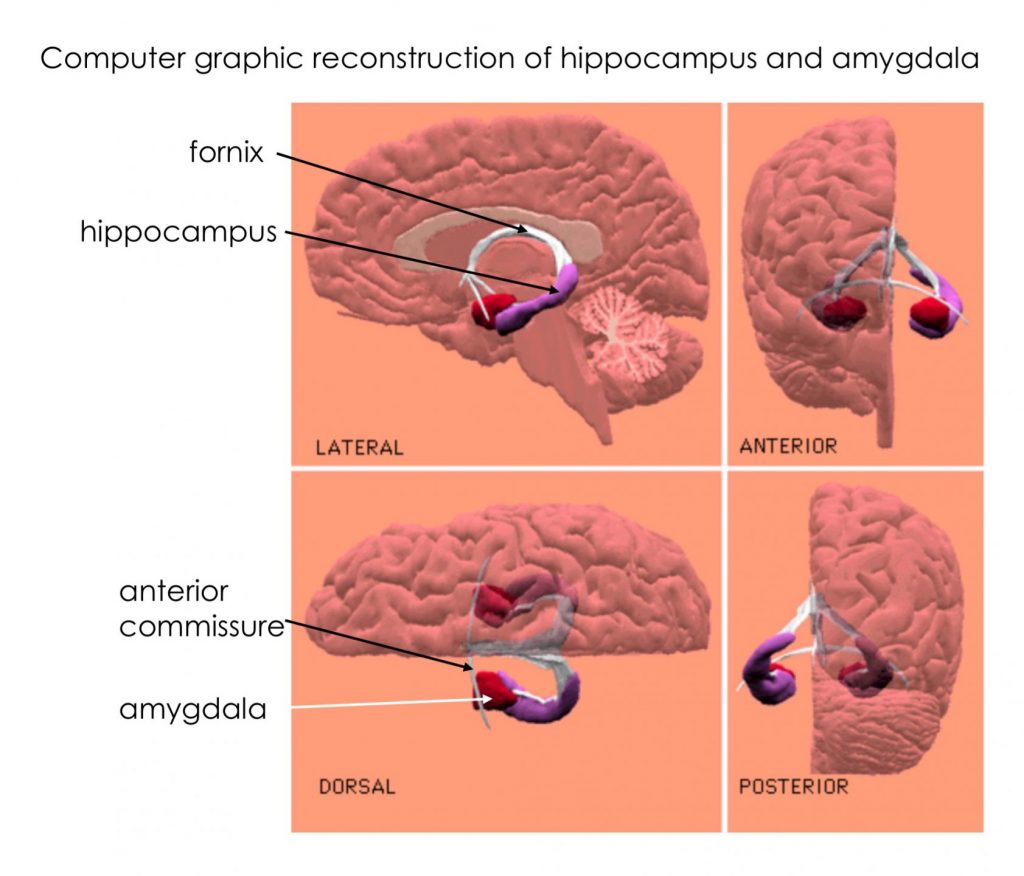
The exercises on the dissections and axial sections below highlight the c-shape of the hippocampus and its outflow tract, the fornix, and some of the relationships among the limbic structures
Circuitry of Hippocampus and Amygdala
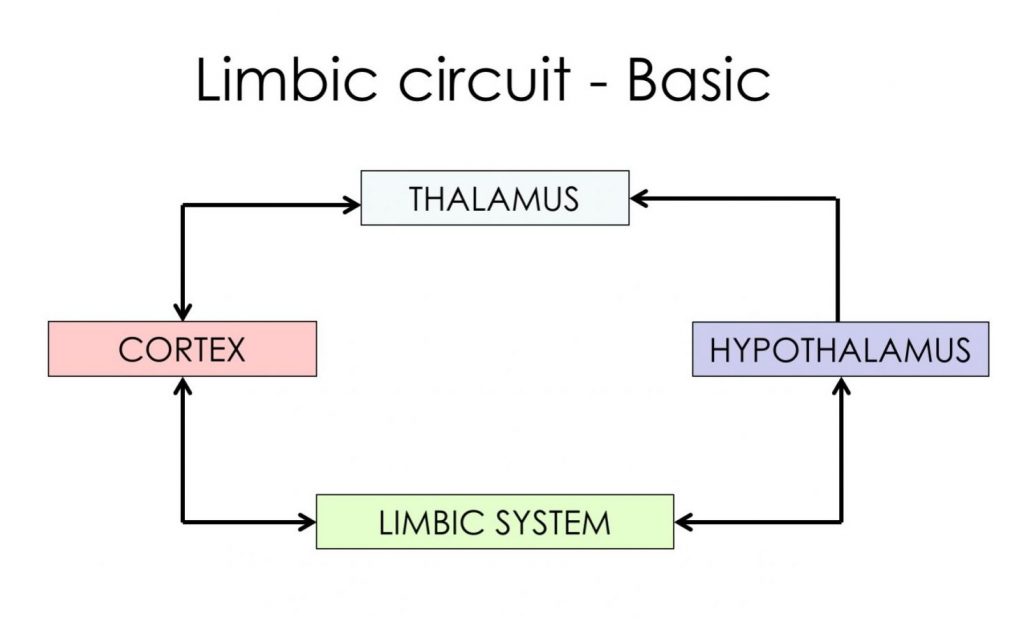
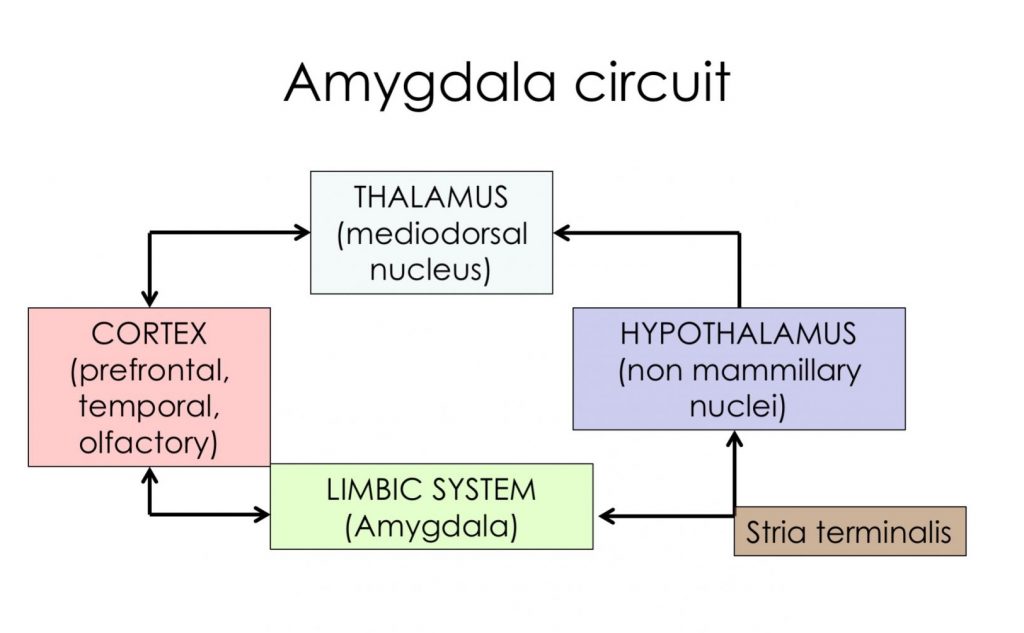
The basic circuit loop for the limbic system runs from cortex to limbic system to hypothalamus to thalamus and back to cortex.
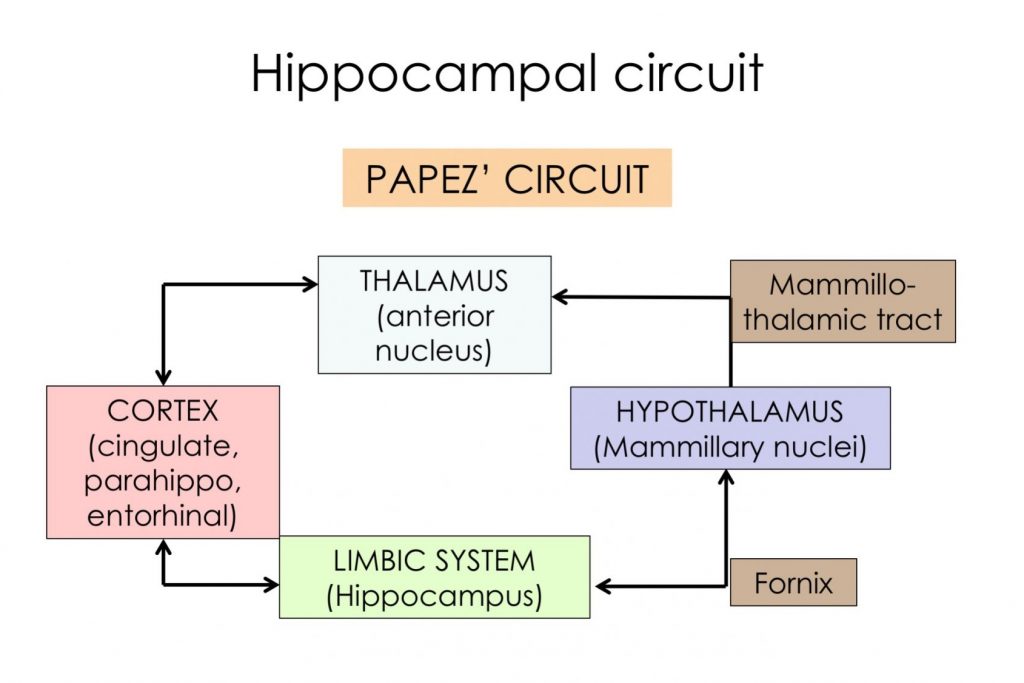
There are 2 major parallel “refinements” of this: one circuit through the hippocampus, involves the fornix and a projection mainly to the mammillary bodies of the hypothalamus, and the anterior nucleus of the thalamus. This is called Papez’ circuit and activity in it is responsible for consolidation of new declarative memories. Damage anywhere in this loop results in impaired consolidation of new declarative memory as exemplified by patient HM. This patient underwent bilateral removal of the hippocampus to control severe epilepsy. Following the surgery, his intelligence was intact, and former memories, but he was unable to create new declarative memories. His procedural memory (eg learning to do a puzzle or master a physical skill) was not affected. This latter type of memory is believed to involve the cerebellum and basal ganglia.
The second loop circuit runs through the amygdala (for emotional memories and behavior), involves the stria terminalis (and other paths) and different parts of the hypothalamus and thalamus and cortex than the circuit for the hippocampus. Of course, things are not so segregated: both the hippocampus and amygdala are highly interconnected.
The amygdala is important in assigning an emotional value to a particular sensory stimulus; it appears to be especially involved in negative emotions like fear and anxiety.
It gets significant sensory input from all modalities. Lesions of the amygdala lead to flat affect and fearlessness. Stimulation of the amygdala in awake patients has been reported to induce feelings of anxiety and fear.
Kluver-Bucy syndrome, best understood in non-human primate research models, refers to the presentation that results from bilateral damage to the medial temporal lobe (especially the amygdala). It is characterized by flat affect, fearlessness, inappropriate sexual behavior, hyperorality, and visual agnosia. In humans the syndrome can be more subtle. Patient SM is a well studied research subject who has a disease (Urbach-Wyethe disease) that causes degeneration of the amygdalae bilaterally.
Thalamus
The thalamus is a collection of nuclei in the diencephalon. It is roughly an egg shape making up the upper wall of the 3rd ventricle, with two posterior protrusions (LGN and MGN) that overhang the superior colliculi. It is bounded laterally by the posterior limb of the internal capsule, and anterolaterally is the caudate. Anteroinferiorly is the hypothalamus and posteroinferiorly is the subthalamic nucleus. Its major role is to relay information to the cortex. It is worth mentioning that a major source of input to the thalamus is from the same region of cortex to which to projects.
Please review the first 2 labs to remind yourselves of the location of the thalamus (on either side of the upper part of the third ventricle), and complete this table by dragging and dropping the nuclei and cortical locations into their correct place.
Structures to Identify