
2 Lab Week 2: Internal Brain Morphology
Learning Objectives
1. Describe the anatomy of the ventricles of the brain, including their parts, shape, position in the brain, and neighboring structures.
Predict the cross sectional shape of the ventricles in coronal and horizontal sections.
Identify the following deep nuclear structures of the brain and describe their relationship to the ventricles: caudate, thalamus, putamen, hypothalamus, hippocampus, amygdala.
2. Describe the formation, circulation pattern and absorption of cerebrospinal fluid (CSF).
Locate the choroid plexus and arachnoid villi and describe their function.
Trace the potential flow paths of a molecule of CSF from its origin in the choroid plexus of the lateral ventricle, through the ventricular system and subarachnoid space, to its absorption through arachnoid villi into the superior sagittal dural venous sinus
Describe the location of the lumbar cistern and state its clinical significance.
Predict the consequences of CSF blockage in the infant and adult brain.
3. Describe the anatomy of the internal capsule.
Identify and name the 3 major parts of the internal capsule – anterior limb, genu, posterior limb- and the gray matter structures that neighbor them.
This week our task is to become familiar with the challenging internal anatomy of the brain. Unlike the spinal cord which has a regular H-shaped pattern of gray matter surrounded by white matter throughout its length, the brainstem and forebrain are filled with irregular clumps (nuclei) or layers of gray matter, highly enmeshed but homogeneous-looking white matter bundles, and irregularly-shaped ventricle spaces. We hope to help you learn to use the ventricles as a tool for navigating internal structures.
Please note the lab atlas on the canvas course site is a great resource for this topic.
Please also be aware that there is intentional repetition to reinforce your understanding, and we use models, computer reconstructions, special intricate dissections and Nissl stained material to enhance your understanding.
IMPORTANT! As we progress to understanding anatomy through 2D clinical images, a key concept to know now is the convention for presentation in clinical images such as MRIs and CT scans.
In axial (horizontal) images, the orientation is anterior at the top of the page and posterior at the bottom, and the image is viewed from below, as if you were standing at the foot of a bed on which the patient is lying on their back. So, the left side of an axial image is the patient’s right side.
In frontal (coronal) images, the orientation is as though you were facing the patient’s face, so the left side of the image is the patient’s right side.
Be aware, however, that there is no convention for pathological specimens and preserved brain slices, so look for labels if the side is important (eg., in predicting location of symptoms).
Likewise, in histological preparations of brainstem or cord, although anterior is often presented at the bottom of a page and posterior at the top of the page, there is no convention about right and left sides of the specimen, so there is no way to distinguish left from right unless indicated with a label.
Ventricles
The ventricles are a system of cerebrospinal fluid (CSF)-filled spaces within the brain, derived from the lumen of the embryonic neural tube. Choroid plexus in the ventricles creates CSF, which can only exit the ventricular system via openings from the most caudal (4th) ventricle to the subarachnoid space.
Abnormalities in ventricular morphology can be helpful diagnostically. Ventricles can also serve as helpful landmarks to navigate the internal morphology of the brain, when you are viewing clinical images.
Watch this movie which shows
1. 3D reconstruction of ventricles in situ
2. a coronal series of brain slices
3. an axial series of brain slices
Each series of sections highlights the ventricle profiles and identifies their gray matter neighbors.
If you would like to view the video with closed captioning on, please visit this link https://youtu.be/vFE3ZUlvgAU
Neighboring structures
Review Dr. Pradhan’s lectures and the following videos using computer graphic reconstructions, special dissections, and clinical images to demonstrate the ventricles and their neighboring structures. Keep in mind that the horns of the lateral ventricles can be referred to by their anatomical position or by the lobe they are in. Thus, the anterior horn is the frontal horn, the posterior horn is the occipital horn, and the inferior horn is the temporal horn. Also note how close the frontal horns are (separated only by a connective tissue membrane, the septum pellucidum), and how far apart the temporal horns are, lying deep to the parahippocampal gyrus.
Try to develop for yourself
1. a sense of the 3D shape of the ventricles and how the ventricle profiles appear in coronal and axial sections.
2. an understanding of the 3D shape, size and disposition of the structures that neighbor the ventricles.
There is some terminology used that is a bit advanced for us at this point in the course, including parts of the corpus callosum (genu anteriorly and splenium posteriorly), the fimbria and column of the fornix, the optic tracts, the nucleus accumbens (important in addictive behavior), septal nuclei, the claustrum, mammillothalamic tract. Allow yourself to hear the terms, but do not stress about these details at this time. You might like to return to these videos later in the course. The structures you need to know for this lab are listed at the end of the chapter and are emphasized in the interactive exercises.
Basal Ganglia
Deep to the subcortical white matter lies the gray matter comprising the basal ganglia (major components: caudate, putamen, globus pallidus) and the diencephalon (major components within the cerebral hemisphere: thalamus, hypothalamus). Terminology is the first thing to deal with: the caudate and putamen comprise the striatum, and the putamen and globus pallidus comprise the lentiform nucleus.
Amygdala and Hippocampus
The amygdala, an almond shaped nucleus, is part of the limbic system within the medial temporal lobe. It lies predominantly anterior to the inferior horn of the lateral ventricle. It is seen only in very anterior sections through the temporal lobe in the coronal plane and in very inferior sections in the axial plane.
The hippocampus is 3 layered cortex that lines almost the full extent of the medial surface of the inferior horn of the lateral ventricle, hence it is seen in many more sections than the amygdala is seen in any series of sections through the temporal lobe.
Students sometimes have difficulty distinguishing the hippocampus from the amygdala. One morphological feature to keep in mind is that the amygdala is a nucleus and relatively uniform in its density, while the hippocampus is 3 layered cortex composed of layers of gray and white matter and thus appears stripy and squiggly.
Consolidate your knowledge by completing the exercises.
Cerebrospinal Fluid
CSF is a colorless fluid created by choroid plexus within the lateral, 3rd and 4th ventricles.
Choroid plexus is a complex structure consisting of arterioles, pial cells and ependymal cells (cells that line the ventricles). It produces CSF from arterial blood by active transport and filtration. About 500mls of CSF is produced each day.
CSF flows passively through the ventricular system and exits to the subarachnoid space via one median and 2 lateral exit foramina in the 4th ventricle. CSF circulates around the brain and cord in the subarachnoid space, cushioning those structures, and providing a route for transfer of metabolites from interstitial fluid away from neurons in the CNS, into the ventricles across the ependymal cells, and back into the venous system.
Where the surfaces of the brain and cord are highly irregular, with an concomitant increase in the distance between the pia and arachnoid, expansion of the subarachnoid space is called a cistern. Several of these exist around the brain, but the most important one clinically is the lumbar cistern formed between the end of the spinal cord and the continuation of the arachnoid to form a sac inferior to the L2 vertebra. From this cistern, CSF can be sampled for diagnostic evaluation in a lumbar (or spinal) tap. It is important to access the space below the L3 vertebra to avoid the possibility of damaging the cord. The fibers of the cauda equina (dorsal and ventral roots of spinal nerves) occupy this cistern, but slide away from the needle as it is inserted.
Hydrocephalus results from an excess of CSF, due to an imbalance in the production vs absorption of CSF. It can become life-threatening if unrelieved, as the resulting increase in intracranial pressure can cause the brain to herniate. If hydrocephalus is untreated in an infant, it may lead to enlargement of the skull, as the sutures have not yet formed and membranous tissue between the individual skull bones can stretch to accommodate the increased volume to some extent.
Non-communicating hydrocephalus occurs when there is a blockage within the ventricular system (typically at the narrow cerebral aqueduct) that prevents CSF from reaching the subarachnoid space. CSF accumulates upstream from the blockage and can cause ventricular enlargement. Communicating hydrocephalus results from insufficient drainage through the arachnoid villi; this can occur due to scarring from meningitis, for example.
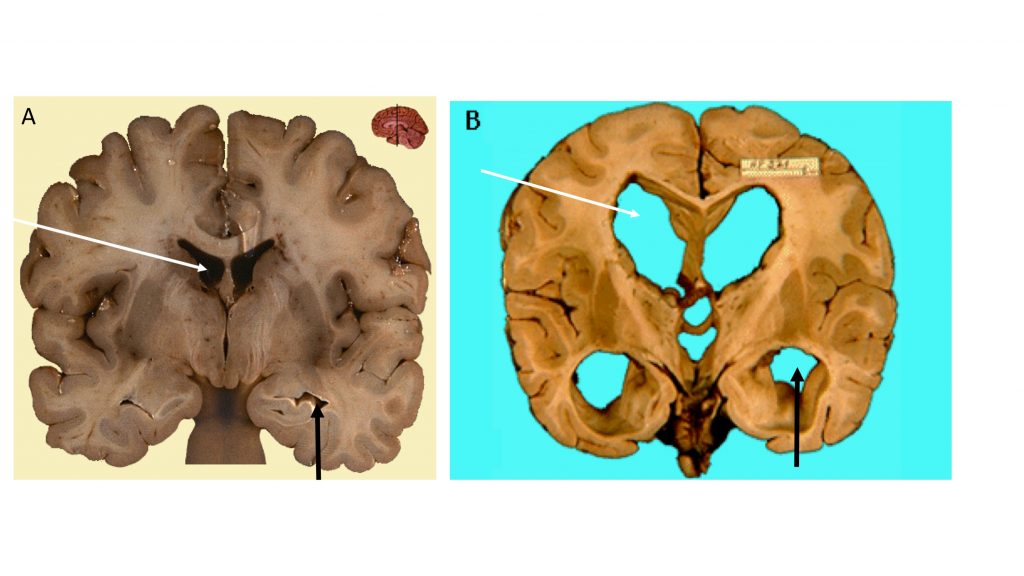
The image below shows postmortem coronal slices in approximately the same plane, through a normal brain (A) and a brain from a patient with severe hydrocephalus (B). Notice the difference in size of the lateral ventricle anterior horns (white arrows) and the inferior horns (black arrows).
Note also that ventricles will enlarge if there is loss of brain tissue, as occurs in some dementias and brain injuries.
 Internal Capsule
Internal Capsule
The internal capsule is a clinically important part of the white matter, composed of axons connecting the cerebral cortex with subcortical structures. These axons, to and from wide swaths of cortex, are funneled down between the deep gray nuclei of the basal ganglia in the core of the cerebral hemisphere. Strokes (cerebrovascular accidents or CVAs) affecting especially the posterior limb of the internal capsule can have devastating effects on motor and sensory function.
The figure below is a dissection from the lateral aspect of the left hemisphere: the cerebral cortex of the frontal, parietal and temporal lobes and the insula, along with the lentiform nucleus, have been removed to show the continuity of the internal capsule with the white matter of the cortex superiorly. Some of the fibers from the posterior limb and genu continue caudally through the cerebral peduncle; you can trace them in the dissection.
The internal capsule has several parts: the anterior and posterior limbs and the genu are more or less in the same axial plane, while the sublenticular and retrolenticular parts are inferior and posterior, respectively, to the lentiform nucleus (ie putamen and globus pallidus).
The caudate lies medial to the anterior limb of the internal capsule rostrally, and the thalamus lies medial to the posterior limb more caudally. The lentiform nucleus is lateral to both limbs.
Familiarize yourself with these views of the internal capsule in MRIs. The posterior limb carries important somatosensory fibers ascending to cortex, and motor tracts descending to the brainstem and spinal cord (notably the corticospinal tract – more on this later); thus damage to the posterior limb can lead to significant impairment in motor function in the opposite side of the body. In the figure on the right, the part of the internal capsule shown in yellow has to be the anterior limb, because you recognize that it is between the caudate and lentiform nuclei.
This is a lot of new information! Please be assured that we will be revisiting this content when we explore the sensory and motor systems of the brain. Become familiar with the terms and learn what you can now, and you can review and consolidate in upcoming chapters and labs. The material we learn in these first few weeks provides a foundation for the rest of the course.
As you view the following 2 movies, keep in mind the key relationships, which will help you navigate the internal morphology of any section you come across.
MRI Axial Series
MRI Coronal Series
Try these exercises to help you put it all together and consolidate what you know.
In the following two exercises, study each image (focus on identifying midline structures) and try to imagine the correct plane on the mid-sagittal view of the brain, and on the model of the ventricles by considering the ventricular profiles in each image and matching those to points on the model. Clicking on the “i” symbol shows the answer, and provides a description of the section.
We recommend using full screen view when it is available (see symbol top right).
And here are a few identification practice exercises. Make sure to read the hints (blue “i”) to solidify relationships, and use full screen view when available. And remember, the lab atlas is your trusted friend!
Structures to Identify
Enrichment:
Here are a couple of websites for those of you who want to take a deeper dive: you will be able to see planes of section and can choose labeled or unlabeled views and matching MRIs in many cases.
UBC brain slices with selected labeling and correlated MRIs
Coronal (frontal) series: http://www.neuroanatomy.ca/coronals.html
Horizontal (axial) series: http://www.neuroanatomy.ca/horizontals.html