
19 Urinary System Anatomy
In this chapter we will look at the gross anatomy of the kidney and the urinary tract. The key structures in the urinary system are the kidneys, ureters, bladder, and urethra.
Structure of the Kidney
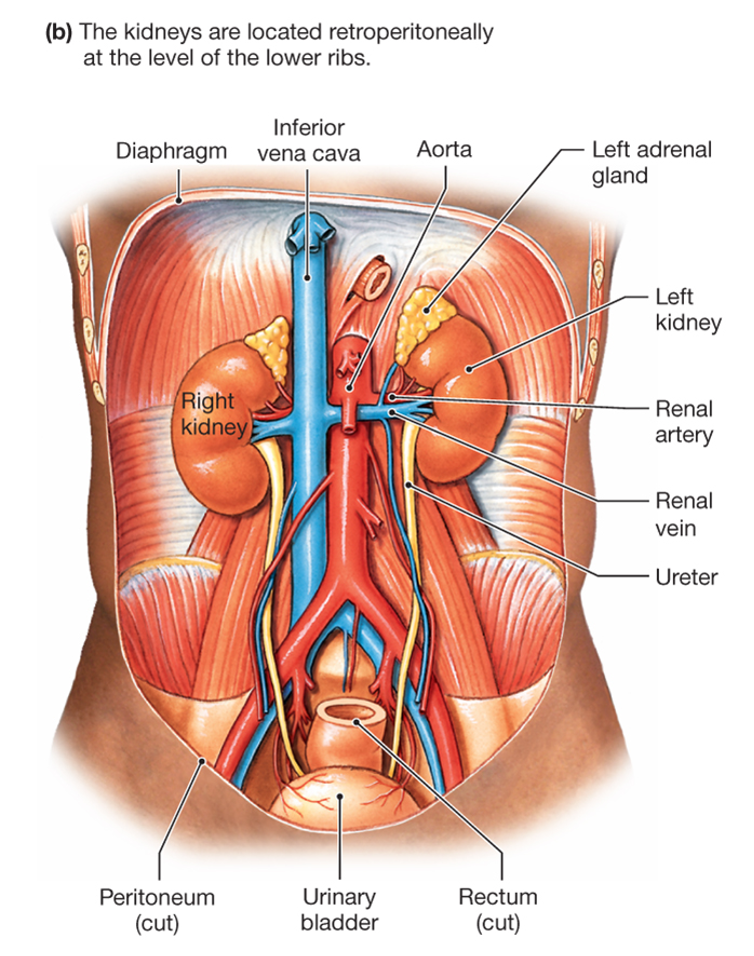
The kidneys are bean-shaped organs lying in the posterior upper region of the abdominal cavity.
The function of the kidneys is the homeostatic regulation of the extracellular fluid. The functional unit within the kidney is the nephron. The schematic figure below depicts the kidney as it would look if sectioned along its long axis and shows how the nephrons are arranged between the two major regions of the kidney, the cortex and the medulla.
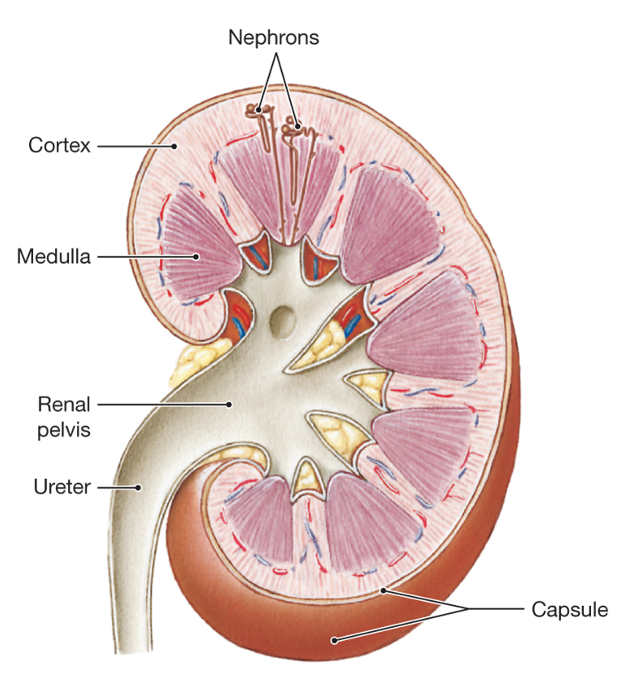
The tissue of the kidney (also called the parenchyma) is divided into two basic regions: an outer cortex, and an inner medulla. As you will see, certain parts of each nephron are located in the cortex, and certain parts are located in the medulla.
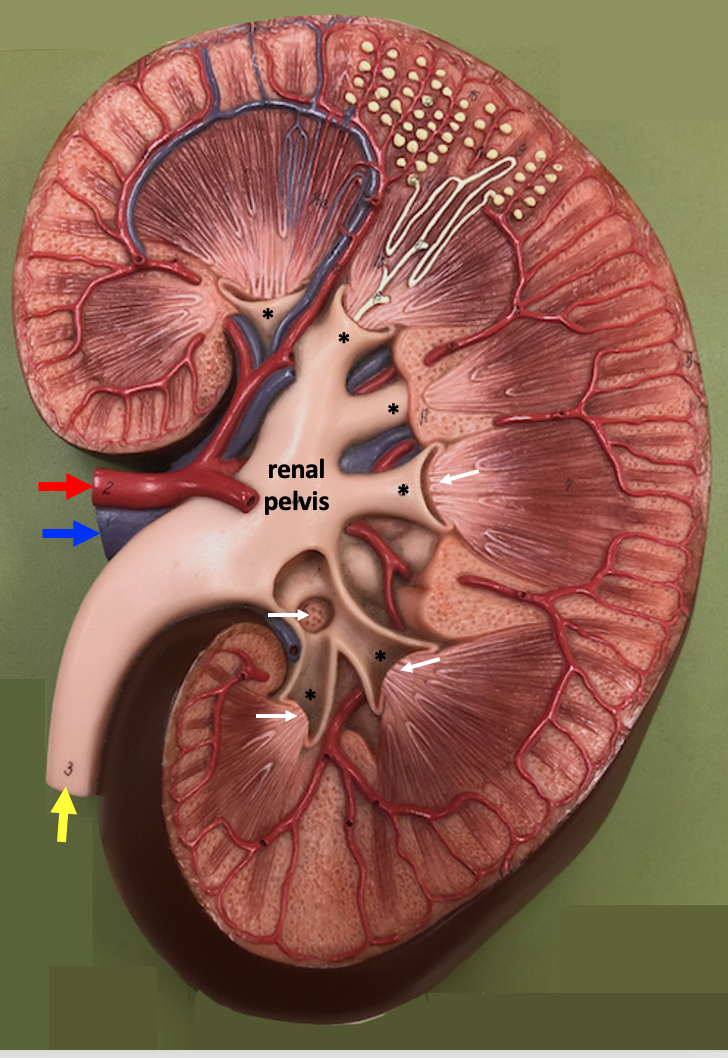
We will be studying the anatomy of the kidney using the model shown below. Similar to the figure above, the model depicts a kidney sectioned along its long axis.
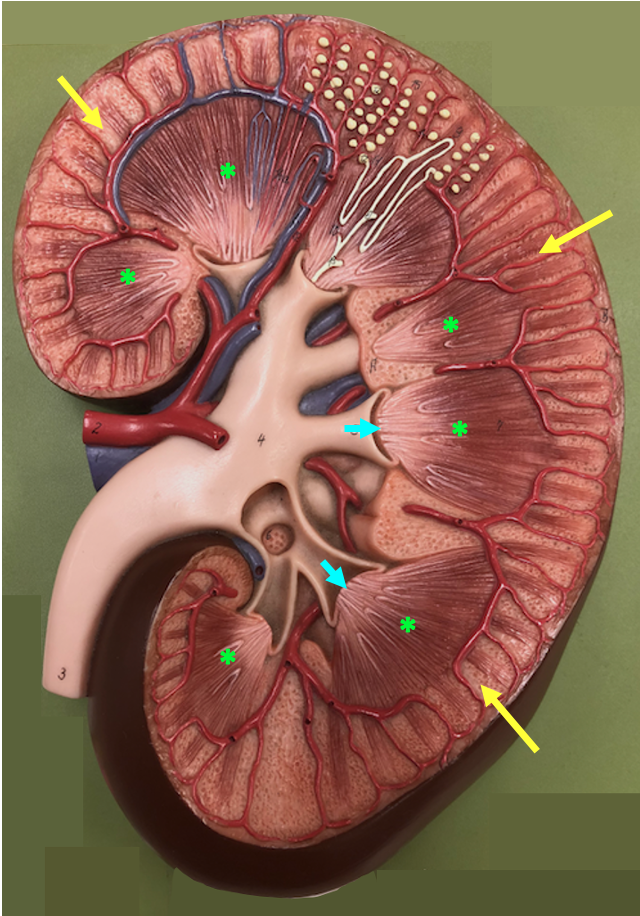
At the gross level, the medulla contains dark structures called pyramids. The pyramids are formed by many parallel tubules and capillaries. The cortex is the outermost region, under the connective tissue capsule that surrounds the kidney.
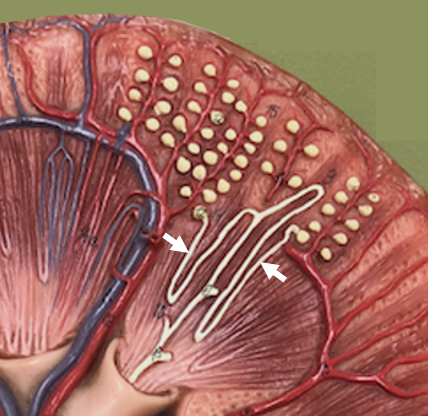
The figure below shows a detail of the region of the model where two nephrons are depicted. Nephrons are microscopic structures and would not normally be visible at the gross level, but this detail effectively illustrates how nephrons are distributed between the cortex and the medulla. The nephron has an initial ball-shaped structure called the renal corpuscle. Renal corpuscles are only found in the cortex. The renal corpuscle attaches to the renal tubule that forms the rest of the nephron. The renal tubule is formed by a simple epithelium and has a convoluted shape, moving out of and back into the cortex. The last part of the renal tubule, the collecting duct, forms a tube that runs vertically through the cortex and medulla and ends at the papilla, the cone-like structure at the tip of each renal pyramid.
Urine forms in the nephrons and drains from the papilla into the collecting system, which collects urine and delivers it to the bladder. The first part of the collecting system is the calyx (plural: calyces), a cup-like structure that fits around the papilla. The calyces form short branches that attach to a wide space called the renal pelvis. The renal pelvis then narrows to form the ureter, a tube that conveys urine to the bladder where it is stored.
The figure below is an X-ray image of the ureter, pelvis, and calyces.
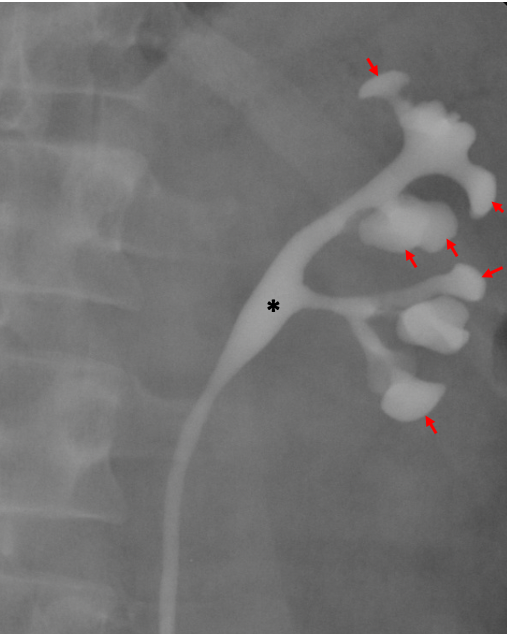
The ureter and the renal blood vessels (renal artery and renal vein) are all found at the hilum of the kidney. The hilum is the region on the concave surface where stuff enters and exits the organ. Other structures with a hilum are the lung, or a bean seed (the root and shoot form at the hilum of the seed when it sprouts).
The figure below shows the renal model again, with an emphasis on the blood vessels and the collecting system.
The calyces, renal pelvis, ureters, and bladder are all lined with a specialized type of epithelium called uroepithelium (or transitional epithelium). The uroepithelium is a stratified epithelium with tight junctions between adjacent cells so that it acts as an important permeability barrier. Urine can be made more concentrated than the extracellular fluid, so it is important that the structures that conduct and store urine don’t allow water to be drawn into the urine. Another unique feature about the uroepithelium is that the epithelium can stretch when the bladder is full and its walls are distended.
This following video from Acland’s Video Atlas of Anatomy is very helpful for understanding and reviewing kidney anatomy. It is optional because I won’t be testing you using images from the video.
Structures in the Urinary Tract
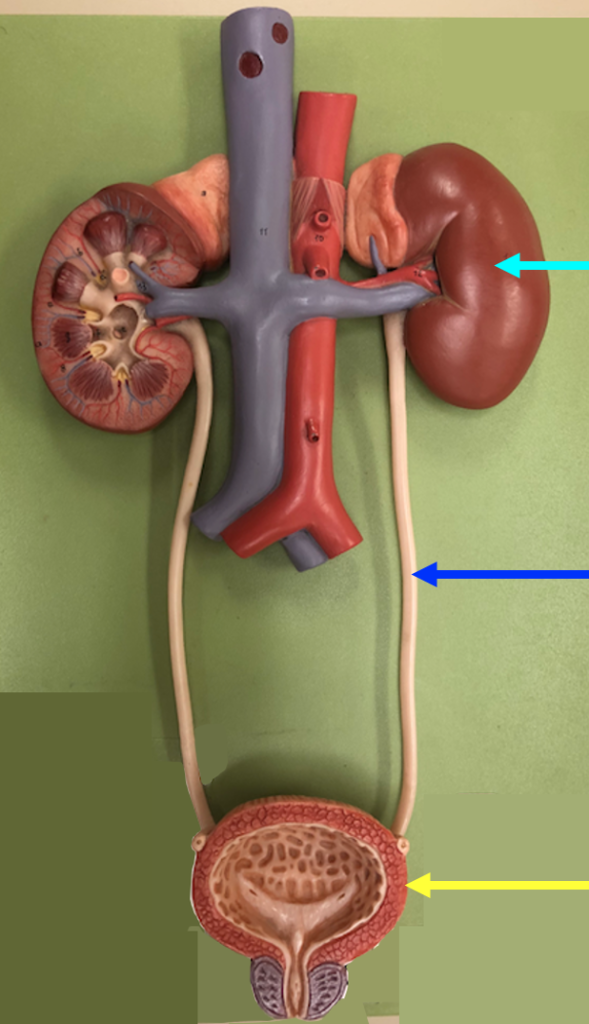
The full urinary tract can be seen in the model shown in the next figure.
Focussing on the top part of the model, we can see the renal vein and the renal artery connecting to the large vessels in the abdomen.
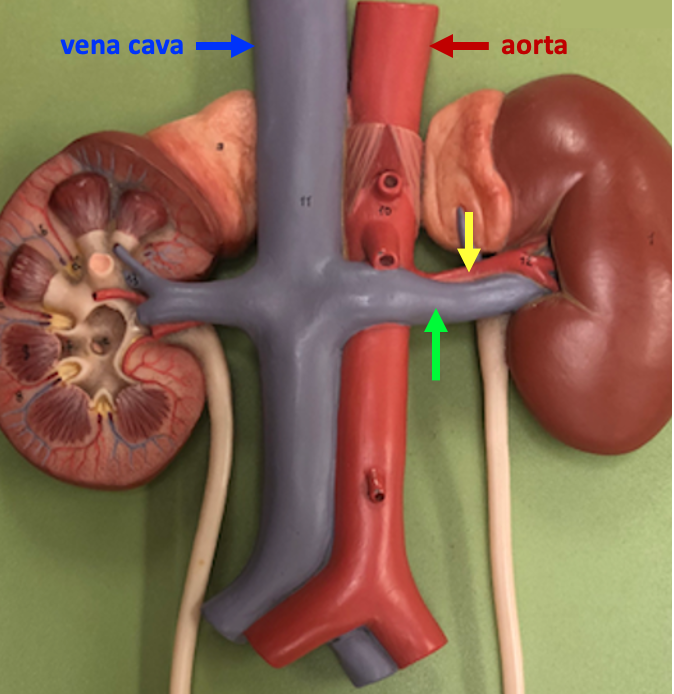
The renal artery receives blood from the aorta, the major artery that carries blood away from the heart. The renal vein, which lies anterior to the renal artery, carries blood away from the kidney directly to the inferior vena cava, the major vein that returns blood from the lower part of the body to the heart. The inferior vena cava lies on the right side of the body because it returns blood to the right atrium of the heart. As a consequence, the left renal vein is a bit longer than the right renal vein.
Urine that forms in the kidneys is carried to the bladder via the ureters. In the model, the bladder is sectioned to reveal its interior surface on the posterior wall.
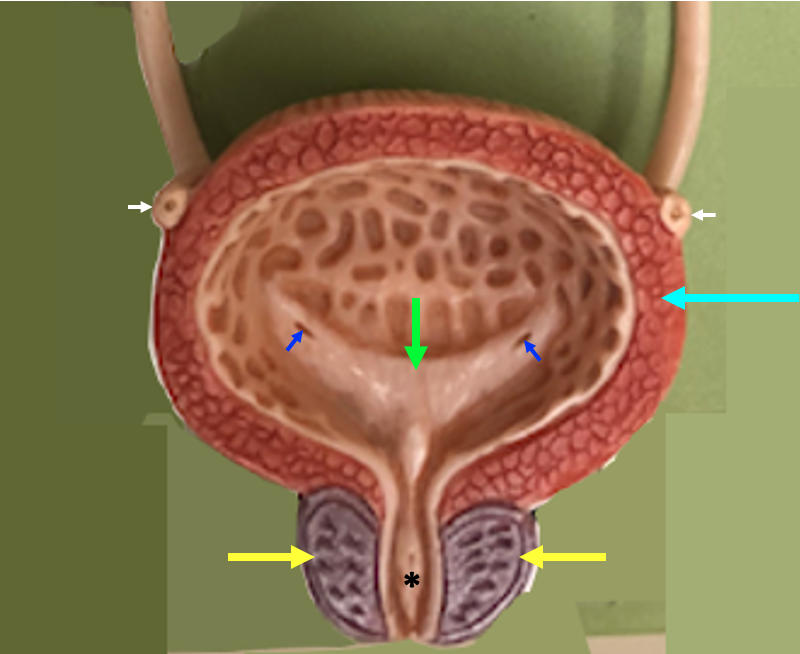
The bladder is a hollow organ whose walls contain layers of smooth muscle known as the detrusor muscle. On the posterior wall of the bladder is a thickened, triangular region known as the trigone. The trigone is positioned above the urethra, the bladder outlet, and has a slit on each side, which is the narrow opening of the ureter. This model depicts the male anatomy, with the prostate gland sitting below the bladder and surrounding the first part of the urethra, called the prostatic urethra in males.
The next figure compares the female and male anatomy of the lower urinary tract.
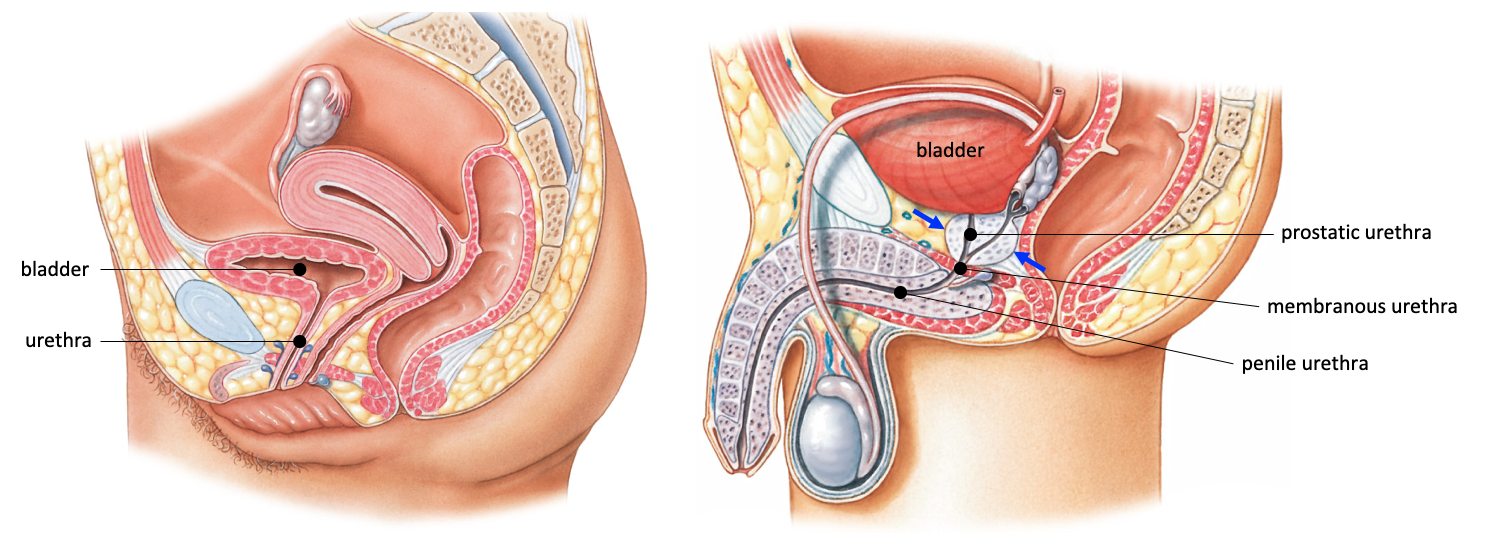
In the female, the urethra is quite short, averaging only a few centimeters. In males, the urethra is much longer, and divided into three segments. The initial part of the urethra, the prostatic urethra, travels through the prostate gland (blue arrows). The membranous urethra travels through skeletal muscle at the floor of the pelvis, and the much longer penile urethra is found within the penis.
Clinical Example: Drug Treatments for Benign Prostatic Hyperplasia
As men age, many will experience non-cancerous growth of the prostate gland called benign prostatic hyperplasia. Benign prostatic hyperplasia can cause difficulty in urination because the enlarged prostate presses on the urethra. Common symptoms are increased frequency of urination, difficulty in starting urination or fully emptying the bladder, and a weak flow of urine.
The prostate gland is in a difficult place to access surgically, so the typical initial treatment for benign prostatic hyperplasia is with drugs.
- One type of drug treatment promotes relaxation of smooth muscle surrounding the bladder outlet and urethra. Smooth muscle in the urethra and prostate gland is innervated by sympathetic postganglionic neurons, which release the neurotransmitter norepinephrine. Norepinephrine binds to alpha-adrenergic receptors in this location and excites smooth muscle contraction. Thus, alpha-adrenergic antagonists that block this excitation are used to relax smooth muscle and promote urine flow. An example is tamsulosin (FlomaxTM).
- In some cases, the prostate gland volume is much increased, so treatment that limits further prostate growth is desirable. The prostate gland grows in response to a type of androgen hormone known as dihydrotestosterone (DHT). The enzyme 5-alpha reductase converts testosterone to the more potent DHT (DHT is more potent because it has a 2x higher binding affinity and a slower dissociation rate from the androgen receptor than testosterone). 5-alpha-reductase inhibitors are enzyme inhibitors that reduce the formation of DHT in order to limit prostate growth.