
1 Lab Week 1: External Brain Morphology and Blood Supply
Learning Objectives
1. Identify the major gross anatomical features and meninges of the brain.
List and locate the major parts of the isolated brain visible in an intact specimen and in a mid-sagittally sectioned brain.
List and locate the major sulci and gyri, and the lobes they delineate.
Correlate the major functional areas of the cerebral cortex with anatomic landmarks.
Locate the cerebellum, and the 3 parts of the brainstem (midbrain, pons, medulla).
List and locate the 3 meningeal layers, including the named reflections of the dura mater that partition the cranial cavity.
2. Describe the vascular supply of the brain.
Describe the patterns of cerebral cortex supply by branches of the vertebral-basilar and internal carotid arterial systems.
Sketch and label the parts of the Circle of Willis, indicate the structures they supply, and explain the functional significance of the Circle of Willis.
Locate the major cerebral arteries and dural venous sinuses of the brain in clinical images.
Major gross anatomical features
Here is a reminder from Dr. Pradhan’s lecture about the parts of the brain, so you can review terminology.
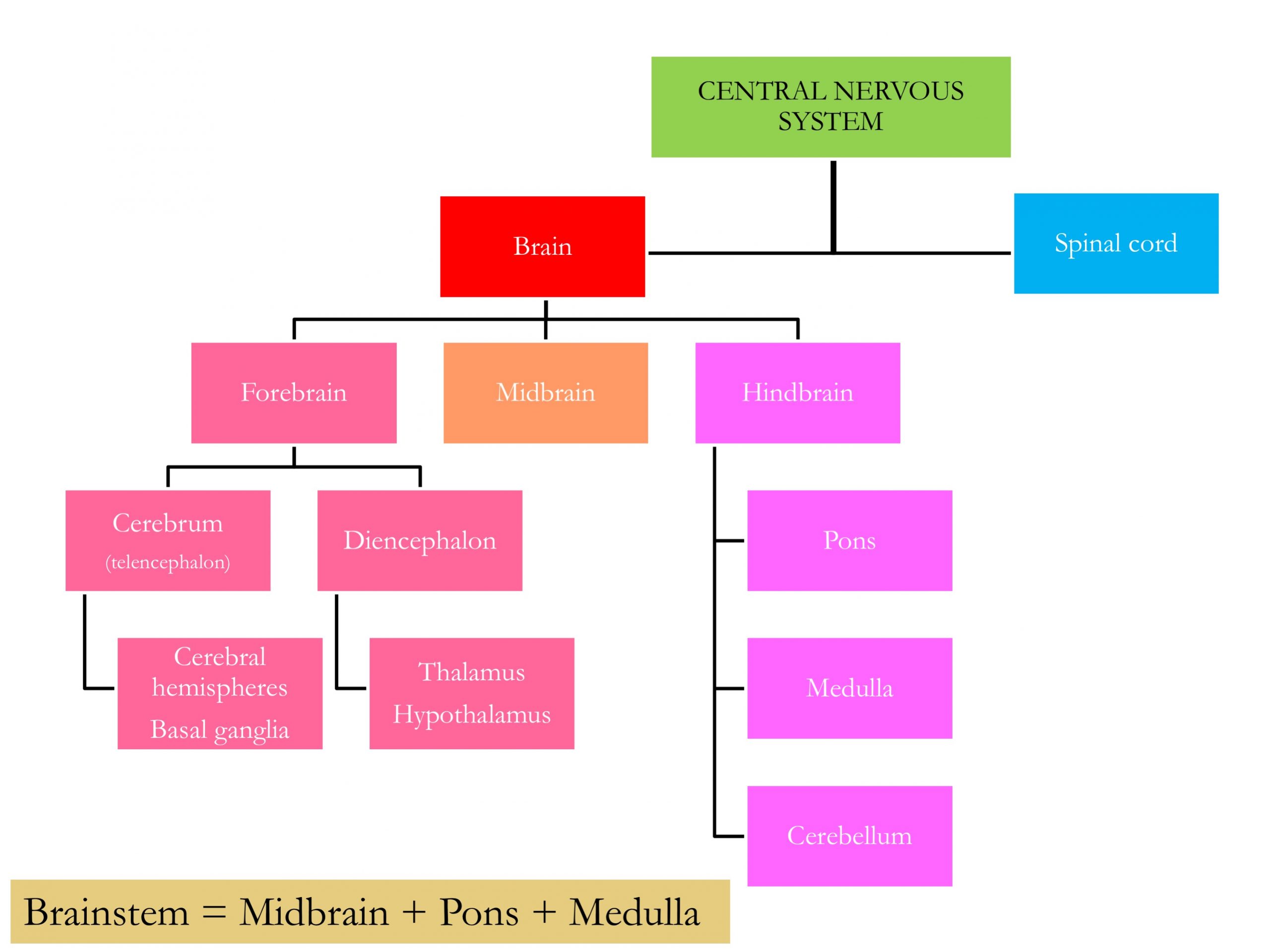
The most salient features of an isolated brain are the left and right cerebral hemispheres, comprised of gyri (convexities) and sulci (grooves) defining lobes. The cerebellum and brainstem are easily visible, and the surface blood vessels are often still intact when we remove brains from our cadaver donors.
Here are two helpful videos demonstrating brain structures.
Please note that we have curated the videos in these lab exercises to match the learning objectives as closely as we can.
In most cases, we have customized the videos by adding interactive features:
- bookmarks (so you can go directly to a particular topic) show up as vertical dashed lines in the video time line. The full list of bookmarks is available if you click on the bookmark tab at the left of the timeline.
- extra information shows up either as “posters” that open directly on the screen as the video plays, and stay for a short period of time, or “buttons”, which require a click to view. Sometimes, we’ve added an image for reference. These are all indicated by open circles along the video timeline at the specific points they show up.
- quizzes can be found within some videos to help you consolidate what you are learning immediately. These are also shown as open circles on the video timeline.
We recommend you view these movies in full screen mode (use the arrows in the right corner of the media). Watch for the extra information and quizzes!
In this video, Dr. Suzanne Stensaas from the University of Utah, provides a guided tour of fixed (preserved) brain and spinal cord, and important information about functional localization. Pay special attention to the central sulcus and the pre-central gyrus (primary motor cortex) and post-central gyrus (primary somatosensory cortex).
Dr. Claudia Krebs, from the University of British Columbia, provides another nice introduction to the CNS in this video. Note that there is some overlap in the material between the two videos.
If you would like to see the original version of the video with closed captions, please use this link: https://youtu.be/kJSCd-2xvW8
Lobes of the brain
After watching the videos. and class lecture, you know that the lobes of the brain are named (mostly) for their overlying bones. The cerebellum (little brain) sits inferiorly to the cerebrum and posterior to the brainstem.
Exercise: Study the animation above, noting which colors represent which lobes or brain parts, then take the quiz.
Match lobes and structures with their corresponding colors
Two entities are called lobes but are not named for overlying bones, and can only be seen with some dissection.
- the insula is seen after dissection of overlying parts of the frontal and parietal cortex (click on the + sign for more information)
- the limbic lobe, composed of the most medial parts of the cerebral cortex, is best seen in a hemisected brain. This figure shows the medial surface of the right hemisphere, and a cut made through the thalamus has removed the brainstem and cerebellum to show the continuity of the limbic lobe comprised of the cingulate gyrus, parahippocampal gyrus and uncus (click on the + signs for more information)
Check your learning!
Drag the label to the correct leader or cortical site.
When you see a blue “i” click on it for more information or a tip!
Of course, cadaver donor brains serve mostly as an aid to build your understanding of the 3D structure that will help you navigate clinical images of living patients that will be a large part of your professional life. Upcoming labs will be focusing on this, but here is a taste of how your knowledge should transfer. Use the slider to move between specimen and clinical views, and labeled and unlabeled views.
Cortical Localization
In this video, Dr. Stensaas demonstrates the functional regions of the cortex (view in full screen mode and look for the extra information)
Test yourself with these exercises! The “answers” are at the end slider position.
Meninges
The meninges are protective connective tissue coverings of the brain that continue inferiorly through the foramen magnum at the base of the skull to surround the spinal cord in the vertebral canal.
Pia mater is the very fine, shiny, almost invisible membrane that follows every contour of the brain parenchyma from gyri down into each sulcus. Arachnoid mater is a white, webby membrane that covers the gyri and spans the sulci—think of shrink wrap! Dura mater is a tough membrane that is often removed from our specimens. It lines the inner surface of the skull, and channels within it form the dural venous sinuses, through which venous blood from the brain is eventually returned to the internal jugular vein. Dura also forms intracranial partitions: the falx cerebri midsagittally between the left and right hemispheres, and the tentorium cerebelli which forms at right angles to the falx and separates the occipital lobe from the cerebellum. The taut free edge of the tentorium delineates the tentorial notch or incisura in which the brainstem sits. In the vertebral canal, dura is not in contact with the vertebra but is surrounded by venous plexuses and fatty connective tissue, through which a catheter can be introduced for delivering epidural anesthesia.
This video is an optional resource, in which Dr. Stensaas presents in depth information on the meninges and on vascular pathology related to meningeal layers and spaces.
Spaces
There is a true space between the arachnoid and pia – the subarachnoid space – in which cerebrospinal fluid (CSF) flows. The large cerebral arteries course through this space before branching and diving into the brain parenchyma. Irregular enlargements of subarachnoid space form cisterns: the most clinically important one is the lumbar cistern from which CSF can be sampled in a lumbar puncture.
Other spaces can can form pathologically, for example, when fluid accumulates and separates adjacent layers. Thus, a bleed can occur that separates the layer of dura from the skull (epidural hemorrhage) or that opens the potential space between the dura and arachnoid (subdural hemorrhage). Bleeding from the large cerebral arteries that run through the arachnoid space can spread through the CSF in that space (subarachnoid hemorrhage).
Blood Supply
Arteries
The brain is supplied by branches of the vertebral-basilar and the internal carotid arterial systems, which unite in the Circle of Willis, a complex of arteries at the base of the brain on the ventral surface of the hypothalamus. The single anterior communicating and the paired posterior communicating arteries unite the anteriorly located internal carotid system and the posteriorly located vertebral-basilar circulations, as well as uniting the circulation of the left and right sides of the brain. Almost the entire lateral surface of the cerebral hemisphere is supplied by the middle cerebral artery (MCA), emerging from the lateral sulcus. The MCA supplies the most anterior part of the temporal pole also. The medial surface is supplied by both anterior cerebral (ACA) and posterior cerebral (PCA) arteries. The parieto-occipital sulcus marks the boundary between these two arterial territories. Note that the anterior cerebral artery follows the upper surface of the corpus callosum and that the posterior cerebral artery supplies the medial aspect of the occipital lobe and the inferior surface of the temporal lobe. Perforating arteries (eg. lenticulostriate arteries) from the Circle of Willis penetrate the brain to supply the deep structures of the cerebrum such as the thalamus, basal ganglia and internal capsule. Branches from the vertebral-basilar system supply the brainstem, cerebellum and anterior part of the spinal cord – the branch names indicate their targets (thankfully!)
In the following clinical images, highlighting arteries, even though you have not been introduced to this sort of image in the course yet, have a go at trying to work out which arteries are which, based on what you know so far. For example, when you see an inverted V shape leading to a single midline artery, that could only be the vertebral arteries joining to form the basilar artery. Similarly, if an artery looks to be supplying the lateral surface of the cerebral hemisphere, that would have to be the MCA. We will see more of these types of images through the course.
Dural venous sinuses
You will not see these in lab specimens, but you can see them in clinical images. Review the images below and note the cavernous, superior sagittal, inferior sagittal, straight, transverse and sigmoid sinuses, and the confluence of sinuses. The intracranial venous system and the venous drainage of the face and scalp are interconnected and can provide a route for transmission of infectious agents, however, the typical drainage from the cranial cavity is to the internal jugular veins forming as the sigmoid sinuses exit the skull.
In the following clinical images, tracer was injected into the carotid system (eg. right internal carotid RICA), then after a time, the blood is imaged in the venous system.
demo for pharm-add gif
demo for pharm: let’s add a H5P item